
Lyme and Other
Tickborne Illnesses
2022 Annual Report
Submitted to the Joint Standing Committee on Health and
Human Services
Prepared by:
Division of Disease Surveillance
Maine Center for Disease Control and Prevention
Maine Department of Health and Human Services

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
1
Introduction and Background
In 2008, during the first special session of the 123
rd
Legislature, hearings and discussion over proposed
legislation regarding the reporting of Lyme disease led to Public Law 2007 Chapter 561. This law, An Act to
Implement the Recommendations of the Joint Standing Committee on Insurance and Financial Services
Regarding Reporting on Lyme Disease and Other Tickborne Illnesses, directed Maine Center for Disease
Control and Prevention (Maine CDC) to submit an annual report to the joint standing committee of the
Legislature having jurisdiction over health and human services matters and the joint standing committee of
the Legislature having jurisdiction over health insurance matters. This annual report is to include
recommendations for legislation to address public health programs for the prevention and treatment of Lyme
disease and other tickborne illnesses in the State, as well as to address a review and evaluation of Lyme
disease and other tickborne illnesses in Maine.
22 MRS, chapter 266-B, was further amended by emergency legislation, introduced as LD 1709 in the 124
th
Legislature, to require the Maine CDC to include information on diagnosis of Lyme disease in its annual
report and to publish related information on its public website.
22 MRS §1645, directs Maine CDC to report on:
1. The incidence of Lyme disease and other tickborne illness in Maine;
2. The diagnosis and treatment guidelines for Lyme disease recommended by Maine Center for Disease
Control and Prevention and the United States Department of Health and Human Services, Centers for
Disease Control and Prevention;
3. A summary or bibliography of peer-reviewed medical literature and studies related to the
surveillance, diagnosis, medical management, and treatment of Lyme disease and other tickborne
illnesses, including, but not limited to, the recognition of chronic Lyme disease and the use of long-
term antibiotic treatment;
4. The education, training, and guidance provided by Maine Center for Disease Control and
Prevention to healthcare professionals on the current methods of diagnosing and treating Lyme
disease and other tickborne illnesses;
5. The education and public awareness activities conducted by Maine Center for Disease Control and
Prevention for the prevention of Lyme disease and other tickborne illnesses; and
6. A summary of the laws of other states enacted during the last year related to the diagnosis, treatment,
and insurance coverage for Lyme disease and other tickborne illnesses based on resources made
available by the federal Centers for Disease Control and Prevention or other organizations.
This is the fourteenth annual report to the Legislature and includes an update on activities conducted during 2022.

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
2
Executive Summary
Lyme disease is a notifiable condition in the State of Maine and, as such, must be reported to the Maine
Center for Disease Control and Prevention (Maine CDC), in accordance with 10-144 CMR chapter 258. The
goal of Lyme disease surveillance is to help define demographic, geographic, and seasonal distribution;
monitor disease trends; identify risk factors for transmission; and promote prevention and education efforts
among the public and medical communities. Effective January 2, 2022, the Council of State and Territorial
Epidemiologists (CSTE) modified the Lyme disease surveillance case definition. Under the new definition,
Maine CDC no longer collects reports of erythema migrans (bull’s-eye) rashes or clinical information on
positive laboratory results from healthcare providers. As a result, Maine CDC epidemiologists classify
reported cases as probable, suspect, and not a case based on laboratory results alone, without the information
on clinical symptoms required under the previous surveillance case definition. Maine CDC no longer reports
confirmed cases of Lyme disease, in line with the CSTE definition. The surveillance case definition is not
intended to be used in clinical diagnosis. Lyme disease surveillance is passive, dependent upon reporting, and
therefore likely to be an under-representation of the true burden of Lyme disease in Maine. Federal CDC
released an updated statement in 2021 that the true burden of Lyme disease may be more than ten times the
number of reported cases. In 2022, federal CDC estimated that the aggregate cost of diagnosed Lyme disease
alone could be $345-968 million to U.S. society.
Maine Tickborne Disease Summary, 2022
●
2,617 probable cases of Lyme disease (preliminary data as of March 8, 2023)
●
824 confirmed and probable cases of anaplasmosis (preliminary data as of March 8, 2023)
●
192 confirmed and probable cases of babesiosis (preliminary data as of March 8, 2023)
●
12 confirmed and probable cases of Hard Tick Relapsing Fever (preliminary data as of March 8, 2023)
●
4 confirmed and probable cases of Powassan virus disease (preliminary data as of March 8, 2023)
* 2022 data are preliminary as of 03/08/2023

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
3
1. The incidence of Lyme disease and other tickborne illness in Maine
Lyme disease
Lyme disease is caused by the spiral-shaped bacteria Borrelia burgdorferi, and, in rare cases, by Borrelia
mayonii, which are both transmitted to humans through the bite of an infected deer or blacklegged tick (Ixodes
scapularis). Symptoms of Lyme disease caused by B. burgdorferi include the formation of a characteristic
expanding rash (erythema migrans) that usually appears three to 30 days after exposure and may appear on any
area of the body. Fever, headache, joint and muscle pains, and fatigue are also common during the first several
weeks. Later features of Lyme disease can include arthritis in one or more joints (often the knee), facial palsy,
meningitis, and carditis (AV block). Lyme disease is rarely fatal. The great majority of Lyme disease cases can
be treated very effectively with oral antibiotics for ten days to a few weeks. Some cases of Lyme disease which
affect the nervous system, joints, or heart may need intravenous antibiotics for up to 28 days.
In 2013, scientists at the Mayo Clinic discovered B. mayonii while testing blood from patients thought to have
Lyme disease with B. burgdorferi infection. Instead, they found a new bacterium that is also transmitted by
deer ticks. Currently, B. mayonii is only found in the Upper Midwest and is not thought to infect ticks in
Maine. Borrelia mayonii causes a similar illness to B. burgdorferi, but can also cause nausea and vomiting;
large, widespread rashes; and a higher concentration of bacteria in the blood. Lyme disease caused by B.
mayonii can be diagnosed with the same tests used to identify Lyme disease due to B. burgdorferi infection
and treated with the same antibiotics.
In the United States, the highest rates of Lyme disease occur across the eastern seaboard (Maryland to Maine)
and in the upper Midwest (Wisconsin and Minnesota), with the onset of most cases occurring during the
summer months. Where they are endemic, deer ticks are most abundant in wooded, leafy, and brushy areas
(“tick habitat”), especially where deer populations are large.
Reported Cases of Lyme Disease – United States, 2020
1 dot placed randomly within county of residence for each confirmed case. High
incidence states highlighted in light blue. Due to the COVID-19 pandemic, 2020
data from some jurisdictions may be incomplete.
Source: U.S. CDC (www.cdc.gov/lyme/datasurveillance/index.html)

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
4
Through 2021, many endemic states no longer count cases of Lyme disease as the burden is too great on the
health department. This affects the national and regional rates as the number of cases appears to drop, though
this is really the result of these health departments using a system to estimate the number of cases rather than
counting each individual case.
Effective January 2, 2022, the Council of State and Territorial Epidemiologists (CSTE) modified the Lyme
disease surveillance case definition. Under the previous surveillance definition, Maine CDC followed up with
healthcare providers to collect corresponding clinical information for every laboratory report received before
the case could be classified as confirmed, probable, suspect, or not a case. Reported erythema migrans rashes
with likely exposure in a state with high Lyme disease incidence were automatically classified as confirmed
cases. Under the new surveillance definition, Maine CDC no longer collects reports of erythema migrans
rashes or clinical information on positive laboratory results from healthcare providers. As a result, Maine CDC
reports cases that meet laboratory evidence alone, without needing healthcare providers to report clinical
information, and no longer reports confirmed cases of Lyme disease, only probable.
Under the new surveillance definition, Lyme disease case counts may increase by 50-100% compared to
previous years under the old surveillance definition (including 2021 case data) (Kugeler et al. 2022). Under the
previous case definition, epidemiologists classified Lyme disease lab reports as confirmed or probable if the
healthcare provider returned the case report form with clinical information for the patient. As healthcare
providers in Maine only returned these reporting forms approximately 50% of the time, epidemiologists
classified lab results lacking this clinical information as suspect cases. The number of confirmed and probable
Lyme disease cases reported by Maine CDC likely underrepresented the true number of cases that could be
classified as confirmed or probable as a result. Under the new case definition, Lyme disease cases are classified
by lab results alone, without needing corresponding clinical information from healthcare providers, reducing
the number of labs that remained uncounted due to failure of healthcare providers to report clinical information.
The first documented case of Maine-acquired Lyme disease was diagnosed in 1986. In the 1990s, the great
majority of Lyme disease cases occurred among residents of south coastal Maine, principally in York County.
Currently, the Midcoast and Downeast areas have the highest incidence of Lyme disease in the State. Based on
2022 data, seven counties have rates of Lyme disease higher than the State rate (Hancock, Knox, Lincoln,
Sagadahoc, Somerset, Waldo, and Washington).
In 2022, (preliminary data as of March 8, 2023) providers reported 2,617 probable cases of Lyme disease
among Maine residents, which is a rate of 188.9 cases of Lyme disease per 100,000 persons in Maine. This is
a 73% increase from the 1,129 cases in 2021. Twenty-nine percent (29%) of reported cases were from the
Midcoast counties (Knox, Lincoln, Sagadahoc, and Waldo) and 17% were from the Downeast counties
(Hancock and Washington).
Forty-three percent (43%) of cases were female and 57% of cases were male. The median age of cases in 2022
was 59 years of age (average age of 52 years). The age at diagnosis ranged from less than 1 to 100 years of
age. For further Lyme disease statistics in Maine, please see Appendix 1.
Maine CDC Report to Maine Legislature on Lyme Disease - 2023
5
Other tickborne diseases in Maine
Anaplasmosis:
Anaplasmosis is a disease caused by the bacterium Anaplasma phagocytophilum, which infects white blood
cells (neutrophils). Anaplasmosis was previously known as human granulocytic ehrlichiosis (HGE) or human
granulocytic anaplasmosis (HGA) but was renamed in 2008 to differentiate between two different organisms
that cause similar diseases (anaplasmosis and ehrlichiosis). Signs and symptoms of anaplasmosis include fever,
headache, malaise, and body aches. Nervous system involvement may occur but is rare. Later features of
anaplasmosis can include respiratory failure, bleeding problems, organ failure, and death. Anaplasmosis is
transmitted to a person through the bite of an infected deer tick. As of March 8, 2023, Maine reported 824
confirmed and probable cases of anaplasmosis in 2022, a 2% decrease from the 841 cases in 2022. Cases
occurred in every county in Maine. For further anaplasmosis disease statistics in Maine, please see Appendix 2.
Babesiosis:
Babesiosis is a potentially severe tickborne disease transmitted through the bite of an infected deer tick. Signs
of babesiosis range from no symptoms (asymptomatic) to serious disease. Common symptoms include extreme
fatigue, aches, fever, chills, sweating, body aches, dark urine, and anemia. People who are infected generally
make a full recovery if they have a healthy spleen and do not have other diseases that prevent them from
fighting infections. As of March 8, 2023, Maine reported 192 confirmed and probable cases of babesiosis in
2022, a 4% decrease from the 201 cases in 2022. Cases occurred in every county except Aroostook and
Piscataquis. For further babesiosis disease statistics in Maine please see Appendix 2.
Hard Tick Relapsing Fever:
Hard Tick Relapsing Fever (HTRF), previously referred to as Borrelia miyamotoi disease, is caused by a
species of spiral-shaped bacteria, called B. miyamotoi, that is closely related to the bacteria that causes
tickborne relapsing fever (TBRF). It is more distantly related to the bacteria that causes Lyme disease. First
identified in 1995 in ticks from Japan, two species of North American ticks carry B. miyamotoi, the deer tick
and the western blacklegged tick (Ixodes pacificus). Common symptoms include fever, chills, headache, joint
pain, and fatigue. Although HTRF is not nationally notifiable, U.S. CDC, in association with endemic states,
developed a case classification to standardize reporting and understand the prevalence in the United States.
Hard Tick Relapsing Fever (Borrelia miyamotoi disease) is a notifiable condition in Maine. As of March 8,
2023, Maine reported 12 probable or confirmed cases of HTRF in 2022 in Maine. Cases occurred in
Androscoggin, Cumberland, Hancock, Kennebec, Knox, Lincoln, Penobscot, Sagadahoc, and York counties.
For further HTRF statistics in Maine, please see Appendix 2.
Ehrlichiosis:
Ehrlichiosis is a disease caused by the bacteria Ehrlichia chaffeensis and Ehrlichia ewingii which infect white
blood cells (monocytes and granulocytes). In the United States, most cases are caused by E. chaffeensis.
Ehrlichiosis was previously known as human monocytic ehrlichiosis (HME). Signs and symptoms of
ehrlichiosis include fever, headache, nausea, and body aches. A rash may

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
6
develop, especially in children. Severe illness, especially when treatment is delayed, may include
encephalitis/meningitis, kidney failure, and liver failure. Ehrlichia chaffeensis and E. ewingii are transmitted to
a person through the bite of an infected lone star tick (Amblyomma americanum). Ehrlichiosis is uncommon in
Maine as this tick is not commonly found here. However, as lone star tick populations continue to creep
northward, this disease may become more common in Maine in the future. At present, most cases detected in
Maine are due to exposure to infected ticks during travel to an endemic state. As of March 8, 2023, Maine
reported seven probable cases of ehrlichiosis in 2022 from Androscoggin, Kennebec, Knox, and Lincoln
counties. Maine had one report of Ehrlichia/Anaplasma Undetermined in 2022, which occurs when serologic
testing results in titers that are the same for both Ehrlichia and Anaplasma, making it impossible to determine
which organism was present. For further ehrlichiosis disease statistics in Maine please see Appendix 2.
Powassan virus disease:
Powassan virus disease is caused by either the Powassan virus or deer tick virus, which are transmitted to
humans through the bite of an infected woodchuck tick (Ixodes cookei) or deer tick, respectively. Signs and
symptoms of Powassan virus disease include fever, headache, vomiting, weakness, confusion, seizures, and
memory loss. Long-term neurologic problems may occur. As of March 8, 2023, Maine reported four
confirmed case of Powassan encephalitis in Maine in 2022. This is a record number of Powassan virus
diseases cases in Maine. These cases occurred in Cumberland, Penobscot, Waldo, and York counties.
Spotted fever rickettsiosis:
Spotted Fever Rickettsioses (SFR) are a group of bacterial illnesses, the most common of which is Rocky
Mountain Spotted Fever (RMSF), caused by the bacterium Rickettsia rickettsii. Signs and symptoms of RMSF
include fever, chills, headache, gastrointestinal symptoms, and a non-itchy spotted rash (called maculopapular)
often on the palms and the soles of the feet. Other spotted fever rickettsioses show similar symptoms,
including fever, headache, and rash, and may also feature a dark scab at the site of the tick bite (known as an
eschar). Rocky Mountain Spotted Fever is transmitted to a person through the bite of an infected American dog
tick (Dermacentor variabilis) in most of the U.S. Rocky Mountain Spotted Fever is not known to be endemic
in Maine but could emerge, as American dog ticks are commonly found across the state. As of March 8, 2023,
Maine reported one probable case of SFR in 2022. This case occurred in Lincoln County. For further SFR
disease statistics in Maine please see Appendix 2.
Other emerging tickborne diseases:
U.S. CDC and other researchers are continually on the watch for new or emerging tickborne diseases.
Pathogens emerging in the United States include Bourbon virus, Colorado Tick Fever virus, Heartland virus,
and Ehrlichia muris eauclairensis. While Maine has no documented cases of any of these diseases, there is
serological evidence from whitetail deer of Heartland virus in Maine. Several of these pathogens are transmitted
by ticks that already live in Maine or may move into Maine in the future, so Maine CDC monitors these
pathogens.
Additionally, the Asian Longhorn tick, Haemaphysalis longicornis, which was reported in the U.S. for the
first time in 2017, has been spreading. Already documented in 17 states, the Asian Longhorn tick has been
found in Connecticut, Rhode Island, New York, and Massachusetts, and may find its way to Maine. Though,
compared with other ticks in Maine, the Asian Longhorn tick seems to be less attracted to humans, it has
been found on pets, livestock, wildlife, and humans. In other countries,

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
7
this tick can spread pathogens that make people and animals very sick. Research is ongoing to find out if and
how well these ticks can spread pathogens that cause diseases in the US like Lyme disease, anaplasmosis, and
babesiosis. Maine CDC monitors this research and regional surveillance for the Asian Longhorn tick.
2. The diagnosis and treatment guidelines for Lyme disease recommended by Maine Center for Disease
Control and Prevention and the United States Department of Health and Human Services, Centers
for Disease Control and Prevention
Maine CDC continues to adhere to the strongest science-based source of information for the diagnosis and
treatment of any infectious disease of public health significance. Nationally, the Infectious Disease Society of
America (IDSA) is the leader in setting the standard for clinical practice guidelines on Lyme disease and other
tickborne illnesses.
Lyme disease is diagnosed clinically with the aid of laboratory testing. An erythema migrans (bull’s- eye rash)
on a person from an endemic area is distinctive enough to allow a clinical diagnosis in the absence of
laboratory confirmation. Patients should be treated based on clinical findings. Either a standardized or modified
two-tier testing algorithm (STTT or MTTT, respectively) is recommended for laboratory testing. With STTT,
the first tier includes an enzyme immunoassay (EIA) or immunofluorescence assay (IFA). If this first tier is
positive or equivocal, an IgM and/or IgG Immunoblot follows. The IgM Immunoblot is only considered
reliable if the person is tested within the first 30 days after symptom onset. With MTTT, the first tier uses an
EIA, similar to STTT. If positive or equivocal, a second EIA follows. Acute and convalescent testing, or testing
run on samples collected during illness and after recovery, is useful to determine final diagnosis. Providers
should consider other potential diagnoses for untreated patients who remain seronegative despite having
symptoms for 6-8 weeks, as they are unlikely to have Lyme disease. A diagnosis of Lyme disease made by a
clinician may or may not meet the federal surveillance case definition, and therefore may not always be
counted as a case.
Maine CDC refers physicians with questions about diagnosis to the IDSA guidelines:
www.idsociety.org/practice-guideline/lyme-disease/.
In 2015, IDSA convened a panel to assess and update guidelines for the treatment and prevention of Lyme
disease and other tickborne diseases. The results from this panel were published in the 2020 Lyme disease
guidelines found at www.idsociety.org/practice-guideline/lyme-disease/. This panel affirmed “the term ‘chronic
Lyme disease’ as currently used lacks an accepted definition for either clinical use or scientific study.”
Currently, U.S. CDC recognizes Post-Treatment Lyme Disease Syndrome (PTLDS), defined as symptoms of
pain, fatigue, or difficulty thinking that lasts for more than 6 months after completion of Lyme disease
treatment (https://www.cdc.gov/lyme/postlds/index.html). There is no proven treatment for PTLDS, but U.S.
CDC notes that patients with PTLDS usually get better over time, though this may take many months. The
2015 panel also noted “[Studies] of persistent symptomatology after treatment of verified Lyme disease have
found that prolonged antimicrobial therapy is not helpful and may cause harm. From this, one can infer that
prolonged antibiotic treatment is unlikely to benefit individuals who lack a verifiable history of Lyme disease
while exposing them to significant risk.”

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
8
3. A Summary or bibliography of peer reviewed medical literature and studies related to the surveillance,
diagnosis, medical management, and the treatment of Lyme disease and other tickborne illnesses,
including, but not limited to, the recognition of chronic Lyme disease and the use of long-term antibiotic
treatment
A bibliography of peer reviewed journal articles published in 2022, as related to surveillance, diagnostics,
medical management, treatment, and other topics relevant in Maine for Lyme and other tickborne illnesses is
included in Appendix 3. Maine CDC reviews these journal articles to maintain an understanding of the current
research and literature available on Lyme and other tickborne diseases.
4. The education, training, and guidance provided by Maine Center for Disease Control and Prevention
to healthcare professionals on the current methods of diagnosing and treating Lyme disease and other
tickborne illnesses
Maine CDC continues to emphasize prevention and control of Lyme disease and other tickborne diseases.
Surveillance for tickborne diseases, including Lyme disease, is performed by the Division of Disease
Surveillance, Infectious Disease Epidemiology Program, as anaplasmosis, babesiosis, ehrlichiosis, Hard Tick
Relapsing Fever (B. miyamotoi disease), Lyme disease, Powassan virus disease, and spotted fever rickettsiosis
are notifiable diseases by both medical practitioners and clinical laboratories. Reporting clinicians must submit
subsequent clinical and laboratory information following the initial report. Maine CDC also monitors tickborne
diseases through syndromic surveillance. By querying participating hospital emergency department (ED) patient
visit data, patients that complain of a tick bite are identified. An increase in ED visits for tick bites is usually a
precursor for the typical seasonal increase in incidences of Lyme and other tickborne diseases. A comparison of
2020, 2021, and 2022 syndromic data is included as Appendix 4. Maine CDC performed a spatial analysis of
2022 Lyme disease surveillance data at the county level, showing the geographic spread of the disease in Maine
(Appendix 5).
Outreach and education to clinicians and other healthcare providers is ongoing. Maine CDC epidemiologists
provide consultation to the medical community on tickborne diseases, offering educational and preventive
information as needed. Maine CDC epidemiologists present educational outreach activities and seminars on
tickborne disease prevention targeting the medical community at statewide meetings of school nurses and
others, though the majority of these efforts were conducted virtually in 2022 due to the ongoing COVID-19
response and staffing shortages. Ongoing educational initiatives are featured on the Maine CDC website:
www.maine.gov/lyme.
During 2022, Maine CDC Infectious Disease Epidemiology Program mailed a clinical management guide,
“Tickborne Diseases of the United States: A Reference Manual for Healthcare Providers,” to hospitals, urgent
care providers, and dermatologists. This guide includes information on ticks found in the US and
signs/symptoms, laboratory services, diagnosis, and treatment of twelve tickborne diseases, including Lyme
disease.
●
Maine CDC distributed 172 copies of this guide in 2022
Maine CDC continues to contribute to national surveillance and prevention activities, though these
activities were hampered by ongoing staffing shortages. During 2022, Maine CDC epidemiologists
represented the State at national and regional meetings:
●
CDC Vector Week Conference on Zoom in January 2022
●
Connecticut Agricultural Experiment Station Vectorborne Disease Symposium on Zoom in May 2022
●
Council of State and Territorial Epidemiologists (CSTE) Annual Conference in Louisville, Kentucky in June
2022

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
9
●
CDC Lyme Disease High-Incidence States Meeting on Zoom in October 2022
●
Northeast Epidemiology Conference on Zoom in November 2022
●
Northeast Mosquito Control Association Annual Meeting on Zoom in December 2022
●
Northeast Regional Center for Excellence in Vectorborne Diseases Arbovirus Situational Awareness Calls
(weekly from summer through fall)
●
USDA National Asian Longhorned Tick Stakeholder Calls (monthly throughout year)
●
National Association of Vectorborne Disease Control Officials (NAVCO) Board Meetings
●
NAVCO Regional Calls (throughout the year)
●
NAVCO Membership Calls (throughout the year)
Maine Epidemiologists are active contributors in federal working groups on:
●
Alpha-gal allergy
●
Anaplasmosis
●
Borrelia miyamotoi (Hard Tick Relapsing Fever)
●
Vectorborne diseases
5. The education and public awareness activities conducted by Maine Center for Disease Control and
Prevention for the prevention of Lyme disease and other tickborne illnesses
Maine CDC promotes ongoing educational outreach activities targeting the public and Maine municipalities.
During 2022, Maine CDC epidemiologists provided consultation to the public on tickborne diseases, offering
educational and preventive information as needed. Maine CDC epidemiologists presented educational outreach
activities and seminars on tickborne disease prevention to the general public including:
●
Three presentations or displays held for businesses and community members.
●
Five media interviews given by Maine CDC employees (Infectious Disease Epidemiology Program
Director and Vectorborne Disease Health Educator).
Maine CDC’s Infectious Disease Epidemiology Program Director chairs the State Vectorborne Disease Work
Group; a group comprising both state agencies and private entities, which meets on a bimonthly basis to
proactively address surveillance, prevention, and control strategies. Members of this group include Maine
Department of Health and Human Services; Maine Department of Agriculture, Conservation, and Forestry;
Maine Department of Inland Fisheries and Wildlife; Maine Department of Education; Maine Department of
Environmental Protection; Maine Forest Service; University of Maine Cooperative Extension Services; and the
United States Department of Agriculture. A full list of members can be found in Appendix 6. Educational
efforts by the Vectorborne Work Group in 2022 included:
●
Presentations given on ticks and tickborne diseases
●
Presence in radio and television interviews
●
Distribution of educational materials including Lyme brochures, tick spoons, fact sheets, etc.
●
Formation of a Vector Control District subcommittee to discuss the feasibility and creation of vector control
districts in Maine.
In 2014, Maine CDC created an educational curriculum aimed at teaching students in 3
rd
to 8
th
grade about
tick biology and ecology, tickborne diseases, and tick prevention. The program consists of a twenty-minute
PowerPoint presentation on tick biology and ecology, and tickborne disease information; four ten-minute
interactive activities; and a take-home packet with games, activities, and information for parents.

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
10
In 2022, after the end of the grant cycle that had previously funded the above-mentioned curriculum activities,
Maine CDC shifted focus to maintaining the tickborne disease curriculum. Maine CDC worked with Maine
DOE to distribute the remaining unused stock of physical curriculum materials to interested school nurses and
administrators throughout the state. This resulted in an additional 14 schools in Maine receiving all of the
materials needed to implement the curriculum. Maine CDC plans to review and update the curriculum on the
school curriculum webpage (www.maine.gov/dhhs/schoolcurricula) as needed in 2023.
Educational materials for the 3
rd
-8
th
graders are available online, including an educator’s guide, group
activities, and activity book for both ticks and mosquitoes. Maine CDC included activities and materials in
formats that are useful for distance learning to accommodate a variety of approaches that educators may use for
in-person or virtual settings. Maine CDC continues to review and update the educational materials. Maine
CDC’s interactive workbook called “Take Back Your Yard! A workbook for kids to fight the bite!” is also
available with the curriculum. This workbook is designed for students in 3
rd
-5
th
grades to work with an adult
parent/guardian to identify and remove tick and mosquito habitat around their homes to prevent vectorborne
diseases. Educational materials are available at the following link: www.maine.gov/dhhs/schoolcurricula. As
requested, Maine CDC also makes curriculum materials available for other local, state, and country agencies to
use for tickborne disease education. In 2022, New York City Department of Health reached out to Maine CDC
for permission to reuse parts of the Maine CDC tickborne disease curriculum in a pilot project planned for 2023.
●
The school curriculum webpage (www.maine.gov/dhhs/schoolcurricula) recorded 609 unique
pageviews in 2022.
Maine CDC ran a Social Media Campaign May through July 2022. In previous years, this campaign consisted
of advertisements on YouTube and Facebook, however, the grant cycle that funded those efforts ended prior to
2022. In 2022, Maine CDC produced a campaign that consisted of a series of static ads and short videos on
Facebook, Instagram, and Twitter. Maine CDC added a total of five new social media static ads produced with
a graphic designer to the 2022 social media campaign. These static ads focused on tick identification,
recognition of different life stages of the deer tick (especially nymphs and adults), and EM rash (bull’s-eye
rash) recognition on different anatomical sites and on different skin tones.
Reach and engagement during the campaign include:
●
Facebook (20 Total Posts in Campaign)
○
Total Reach for Campaign: 322,108 (range 79-59,140 per post)
○
Total Post Engagements for Campaign (reactions, link clicks, comments, and shares): 5,031 (range 15-
1,250 per post)
●
Instagram (17 Total Posts in Campaign)
○
Total Reach for Campaign: 8,315 (range 206-1,670 per post)
○
Total Post Engagements for Campaign (reactions, comments, and shares): 198 (range 1-48 per post)
●
Twitter (20 Total Posts in Campaign)
○
Total Reach for campaign: 15,342 (range 432-1,348 per post)
○
Total Post Engagements for Campaign (likes, link clicks, retweets, replies, etc.): 579 (range 6-100 per
post)
Maine CDC maintains a series of short instructional videos to educate the Maine community in tick
prevention and tickborne diseases. All of the instructional videos are available at
www.youtube.com/MainePublicHealth. These videos include:
●
Choosing and Applying Personal Repellents – viewed 29 times in 2022
●
Do You Know Who’s Most at Risk for Lyme Disease – viewed 6 times in 2022
●
How to Choose a Residential Pesticide Applicator – viewed 27 times in 2022
●
How to Perform a Tick Check – viewed 1,196 times in 2022
●
Know How to do Tick Checks – viewed 190 times in 2022

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
11
●
Know How to Prevent Tick Bites – viewed 42 times in 2022
●
Know How to Remove Ticks – viewed 42 times in 2022
●
Reducing Tick Habitat Around Your Home- viewed 120 times in 2022
●
Tick Identification – viewed 1,330 times in 2022
●
Tickborne Diseases in Maine: Anaplasmosis – viewed 562 times in 2022
●
Tickborne Diseases in Maine: Babesiosis – viewed 50 times in 2022
●
Tickborne Diseases in Maine: Lyme Disease-viewed 22 times in 2022
●
Tickborne Diseases: Powassan Encephalitis– viewed 123 times in 2022
Maine CDC’s Lyme disease website is continually updated to provide information to the public and to health
professionals about Lyme disease in Maine. As part of an ongoing effort to review and update Maine CDC
webpages, Maine CDC reviewed and updated the vectorborne disease homepage
(www.maine.gov/dhhs/vectorborne), as well as webpages for seven of the eight endemic vectorborne diseases
in Maine. In 2022:
●
The Lyme disease homepage (www.maine.gov/lyme) received 2,682 unique pageviews.
●
The tick frequently asked questions homepage (www.maine.gov/dhhs/tickfaq) received 1,952 unique
pageviews.
Ongoing educational initiatives featured on Maine CDC’s website include:
●
Anaplasmosis, babesiosis, Ehrlichiosis, Hard Tick Relapsing Fever (Borrelia miyamotoi), Lyme
disease, Powassan virus disease, and Rocky Mountain Spotted Fever fact sheets
●
Tickborne frequently asked questions with peer-reviewed citations
●
Tick identification resources
●
Tick bite and tickborne disease prevention methods
●
Lyme disease, anaplasmosis, ehrlichiosis, and babesiosis Surveillance Reports, selected years
from 2008-2021
●
Vectorborne disease school curricula
●
Maine Tracking Network: Tickborne Diseases
●
Tickborne Diseases in Maine webinar updated annually
During 2022, Maine CDC distributed Lyme disease educational materials to partners and members of the
public. After the close of the grant cycle that funded the bulk of educational material production and distribution
in 2022, Maine CDC will limit the availability of certain materials for public order. This includes tick remover
spoons, which Maine CDC previously offered for order by members of the public and businesses. Going
forward, Maine CDC will reserve the remaining stock of tick spoons for distribution at educational events.
Maine CDC will continue to make all printed materials available for download. Approximate numbers of
materials distributed include:
●
10,417 Wallet-sized laminated tick identification cards
●
16,852 Tick remover spoons
●
953 Lyme disease brochures
●
798 Tick ID posters
●
1,021 What to Do after a Tick Bite posters
●
155 Lyme Disease Awareness Month 2021 posters
●
300 Lyme Disease Awareness Month 2022 posters
●
172 Tickborne Diseases in the United States: A Reference Manual for Healthcare Providers
●
1,754 Prevent Tickborne Diseases bookmark
●
720 Prevent Tickborne Diseases in People and Pets bookmark
●
71 Prevent Tick Bites trail sign

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
12
Members of the Vectorborne Disease Working Group assist Maine CDC in distributing educational materials as
widely as possible throughout the State.
Maine CDC releases Health Alerts (www.maine.gov/dhhs/mecdc/all-health-advisories.shtml), press releases, and
other information on disease concerns of public health significance, including tickborne diseases. Maine CDC also
responds to numerous press inquiries and releases press statements as appropriate. Official releases in 2022 included:
●
Maine CDC Confirms Fatal Case of Powassan Virus in Waldo County (Press Release) – April 20
th
●
2022 Lyme and Other Tickborne Disease Information (Health Alert) – May 9
th
●
Maine CDC Marks Lyme Disease Awareness Month (Press Release) – May 9
th
●
Maine CDC Congratulates 2022 Lyme Disease Awareness Month Poster Contest Winners (Press Release) –
May 19
th
●
Arbovirus Update for Healthcare Providers (Health Alert) – August 3
rd
●
Maine CDC Shares Advice on Home to Avoid Tick Bites This Fall (Press Release) – September 29
th
Pursuant to legislation enacted in the second regular session of the 124
th
Legislature, May 2022 was declared to
be Lyme Disease Awareness Month (PL 2009, chapter 494). Educational activities took place the entire
month including:
• Governor’s Proclamation of Lyme Disease Awareness Month (Appendix 7)
• Information distributed through social media (Facebook, Instagram, and Twitter)
• Information distributed through multiple newsletters throughout the state (medical, veterinary, and other general
interest)
• Information distributed through multiple media interviews across the State of Maine
• Educational tabling event at LL Bean in Freeport, Maine
Another major Lyme Disease Awareness Month activity was the statewide poster contest for students in
grades K-8. Maine CDC asked students to create a poster with the theme “Tick Wise” demonstrating at least
one of the four Lyme disease prevention methods (wear protective clothing, use repellent, use caution in tick
infested areas, and perform daily tick checks). The four winning posters and one honorable mention poster are
available for viewing at the Lyme disease website: www.maine.gov/lyme. Maine CDC used one of the
winning posters for our 2022 statewide educational campaign (Appendix 8). Maine CDC distributed this
poster to schools, state parks, the board of tourism, and historical sites. An online poster gallery of all
artworks submitted over the past thirteen years is available for viewing on Maine CDC’s Lyme Disease
Awareness Month website: www.maine.gov/lyme/month.
In 2012, Maine CDC updated Lyme disease data on the Maine Tracking Network (MTN) Portal, a web-
based portal that allows users to access environmental and health data. In 2018, the Maine Tracking Network
added anaplasmosis and babesiosis data to the Lyme disease portion of the portal. This data portal allows users
to customize their data inquiries from 2001-2020 at the town, county, and state level, and 2021-2023 data
inquiries at the county and state level. The Tickborne Disease portion of the portal was accessed 6,536 times
during 2022. The MTN Tickborne Disease Data is available on Maine CDC’s website at www.maine.gov/idepi.
Please see Appendix 9 for a sample table and Appendix 10 for sample maps. Data can be broken down by:
• Town
• County
• Gender
• Age Group

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
13
In 2018, Maine CDC also launched a Data Dashboard for tickborne diseases on the MTN. This data
dashboard is updated weekly with the rates (per 100,000) and number of cases of Lyme disease, anaplasmosis,
and babesiosis at both the state and county level. This is available as tables, charts, and maps. Case counts
include confirmed and probable cases and data updates occur bi-monthly as Maine CDC classifies new cases.
The data dashboard also includes a trend chart of suspected tick-related emergency department visits by week
and compares the counts to the previous year. The dashboard also includes suspected tick-related emergency
visits as a percent of all emergency visits, allowing for comparison with previous years. Maine CDC obtains
suspected tick-related emergency department visits from hospitals in Maine. This section of the portal received
1,968 visits in 2022. Please see Appendix 11 for a sample trend chart.
Maine CDC’s main prevention message is encouraging Maine residents and visitors to use personal protective
measures to prevent tick exposures. Personal protective measures include avoiding tick habitat, using EPA-
approved repellents, wearing long sleeves and pants, and daily tick checks and tick removal after being in tick
habitats (ticks must be attached >24 hours to transmit Lyme disease). Persons who spent time in tick habitats
should consult a medical provider if they have unexplained rashes, fever, or other unusual illnesses during the
first several months after exposure. Possible community approaches to prevent Lyme disease include landscape
management and control of deer herd populations.
Maine CDC partners with the University of Maine Cooperative Extension Office to monitor the identification
of deer ticks (Ixodes scapularis) in Maine through a passive submission system.
Beginning in April 2019, the University of Maine Cooperative Extension Office offers the testing of deer ticks
for the pathogens that cause Lyme disease, anaplasmosis, and babesiosis. In 2020, the Cooperative Extension
Office added a panel to test non-Ixodes tick species, including the American dog tick and lone star tick for the
pathogens that cause Rocky Mountain Spotted Fever, ehrlichiosis, and tularemia. In 2023, the Cooperative
Extension Office plans to add Powassan and Heartland virus testing to the Ixodes and non-Ixodes panels,
respectively. While the testing of ticks should not be used for clinical diagnosis or medical treatment decisions,
this service provides surveillance information on ticks and tickborne diseases in Maine. For more information
on this service, please visit www.ticks.umaine.edu. Data on the tick submission and tick testing results for 2022
can be found in Appendix 12.
6. A summary of laws of other states enacted during the past year related to the diagnosis, treatment, and
insurance coverage for Lyme disease and other tickborne illnesses based on resources made available
by federal Centers for Disease Control and Prevention or other organizations
Maine CDC performed a search of state and federal legislation. A state-by-state listing of legislation relating
to Lyme and other tickborne diseases can be found in Appendix 13.

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
14
Appendix 1
Maine Lyme disease statistics
Number and Rate per 100,000 persons of Lyme Disease Cases by County of Residence – Maine, 2018-2022*
County
2018
Count
2018
Rate
2019
Count
2019
Rate
2020
Count
2020
Rate
2021
Count
2021
Rate
2022
Count*
2022
Rate*
Androscoggin
68
63.2
98
90.5
40
36.9
64
57.6
76
68.4
Aroostook
4
6.0
2
3.0
4
6.0
3
4.5
12
17.9
Cumberland
288
98.1
354
120.0
178
60.3
226
74.0
350
114.7
Franklin
13
43.5
39
129.1
18
59.6
24
80.8
40
2.9
Hancock
174
317.5
193
351.0
117
212.8
186
331.0
360
640.7
Kennebec
182
149.1
279
228.1
125
102.2
167
134.2
230
16.6
Knox
105
264.0
238
598.4
121
304.2
138
335.9
261
635.3
Lincoln
63
183.4
132
381.1
65
187.7
65
181.4
183
510.8
Oxford
48
83.3
88
151.8
43
74.2
57
97.2
63
107.5
Penobscot
78
51.6
111
73.0
85
55.9
126
82.5
238
17.2
Piscataquis
3
17.9
4
23.8
4
23.8
5
29.1
15
87.4
Sagadahoc
47
131.9
83
231.5
27
75.3
45
121.4
101
272.5
Somerset
45
88.9
68
134.7
37
73.3
80
158.1
125
247.1
Waldo
78
196.5
143
360.1
91
229.1
113
283.1
203
508.6
Washington
15
47.6
31
98.8
33
105.2
38
122.1
93
298.8
York
201
97.5
312
150.3
141
67.9
173
80.6
267
124.4
State
1412
105.0
2175
161.8
1118
84.0
1510
110.0
2617
188.9
*2022 data are preliminary as of 03/08/2023
Note about the data: Effective 01/02/2022, CSTE changed the Lyme disease surveillance case definition to a lab-only definition, which includes only probable cases.
All data prior to 2022 includes confirmed and probable cases. See section Ia for more information.
*2022 data are preliminary as of 03/08/2023
Note about the data: Effective 01/02/2022, CSTE changed the Lyme disease surveillance case definition to a lab-only definition, which includes only probable cases.
All data prior to 2022 includes confirmed and probable cases. See section Ia for more information.
1384
1412
1216
1498
1859
1412
2175
1129
1510
2617
0
300
600
900
1200
1500
1800
2100
2400
2700
3000
2013 2014 2015 2016 2017 2018 2019 2020 2021 2022
Number of Cases
Lyme Disease Cases - Maine, 2013-2022*

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
15
*2022 data are preliminary as of 03/08/2023
Note about the data: Effective 01/02/2022, CSTE changed the Lyme disease surveillance case definition to a lab-only definition, which includes only probable cases.
All data prior to 2022 includes confirmed and probable cases. See section Ia for more information.
*2022 data are preliminary as of 03/08/2023
Note about the data: Effective 01/02/2022, CSTE changed the Lyme disease surveillance case definition to a lab-only definition, which includes only probable cases.
All data prior to 2022 includes confirmed and probable cases. See section Ia for more information.
0.0
20.0
40.0
60.0
80.0
100.0
120.0
140.0
160.0
180.0
200.0
2013 2014 2015 2016 2017 2018 2019 2020 2021 2022
Rate per 100,000
Lyme Disease Incidence - Maine, New England, and US, 2013-2022*
Maine US New England
0.0
50.0
100.0
150.0
200.0
250.0
300.0
350.0
400.0
2013 2014 2015 2016 2017 2018 2019 2020 2021 2022
Rate per 100,000 persons
Lyme Disease Rates by Age Group, Maine 2013-2022*
<5 5-14 15-24 25-44 45-64 65+

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
16
Appendix 2
Maine tickborne disease statistics (excluding Lyme disease)
Number of Selected Tickborne Disease Cases by County of Residence – Maine, 2022*
County
Anaplasmosis
Babesiosis
Ehrlichiosis
Ehrlichiosis/
Anaplasmosis
Undetermined
Hard Tick
Relapsing Fever
Powassan
Spotted Fever
Rickettsiosis
Androscoggin
54
11
1
0
2
0
0
Aroostook
1
0
0
0
0
0
0
Cumberland
88
25
0
0
1
1
0
Franklin
18
1
0
0
0
0
0
Hancock
78
23
0
0
2
0
0
Kennebec
87
24
4
1
2
0
0
Knox
94
28
1
0
1
0
0
Lincoln
108
19
1
0
1
0
1
Oxford
31
3
0
0
0
0
0
Penobscot
45
7
0
0
1
1
0
Piscataquis
1
0
0
0
0
0
0
Sagadahoc
38
9
0
0
1
0
0
Somerset
27
3
0
0
0
0
0
Waldo
86
19
0
0
0
1
0
Washington
16
3
0
0
0
0
0
York
52
17
0
0
1
1
0
Total
824
192
7
1
12
4
1
* 2022 data are preliminary as of 03/08/2023
Number of Selected Tickborne Disease Cases– Maine, 2013 - 2022*
2013
2014
2015
2016
2017
2018
2019
2020
2021
2022*
Anaplasmosis
94
191
185
372
663
476
685
443
841
824
Babesiosis
36
42
55
82
118
101
138
66
201
192
Ehrlichia chaffeensis
3
8
5
7
10
19
13
2
4
7
Ehr/Ana undetermined
2
6
1
4
10
9
2
2
0
1
Hard Tick Relapsing Fever
0
0
0
0
6
8
13
12
9
12
Powassan
1
0
1
1
3
0
2
1
3
4
SFR
2
3
1
4
3
10
5
0
2
1
* 2022 data are preliminary as of 03/08/2023

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
17
* 2022 data are preliminary as of 03/08/2023
0
100
200
300
400
500
600
700
800
900
2013 2014 2015 2016 2017 2018 2019 2020 2021 2022
Number of Cases
Anaplasmosis and Babesiosis, Maine 2013-2022*
Anaplasmosis Babesiosis

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
18
Appendix 3
Peer-reviewed medical literature related to tickborne diseases – bibliography: 2022 Diagnostics and
Surveillance
• Bishop A, Borski J, Wang HH, Donaldson TG, Michalk A, Montgomery A, Heldman S, Mogg M,
Derouen Z, Grant WE, Teel PD. (2022). Increasing incidence of spotted fever group rickettsioses in
the United States, 2010-2018. Vector Borne Zoonotic Dis. 22(9):491-497. doi:
10.1089/vbz.2022.0021.
• Blanchard L, Jones-Diette J, Lorenc T, Sutcliffe K, Sowden A, Thomas J. (2022). Comparison of
national surveillance systems for Lyme disease in humans in Europe and North America: A policy
review. BMC Public Health. 7; 22(1):1307. doi: 10.1186/s12889-022-13669-w.
• Bloch EM, Day JR, Krause PJ, Kjemtrup A, O'Brien SF, Tobian AAR, Goel R. (2022).
Epidemiology of hospitalized patients with babesiosis, United States, 2010-2016. Emerg Infect Dis.
28(2):354–62. doi: 10.3201/eid2802.210213.
• Burtis JC, Foster E, Schwartz AM, Kugeler KJ, Maes SE, Fleshman AC, Eisen RJ. (2022).
Predicting distributions of blacklegged ticks (Ixodes scapularis), Lyme disease spirochetes
(Borrelia burgdorferi sensu stricto) and human Lyme disease cases in the eastern United States.
Ticks Tick Borne Dis. 13(5):102000. doi: 10.1016/j.ttbdis.2022.102000.
• Fleshman AC, Foster E, Maes SE, Eisen RJ. (2022). Reported county-level distribution of seven
human pathogens detected in host-seeking Ixodes scapularis and Ixodes pacificus (Acari: Ixodidae)
in the contiguous United States. J Med Entomol. 59(4):1328-1335. doi: 10.1093/jme/tjac049.
• Giménez-Richarte Á, Ortiz de Salazar MI, Giménez-Richarte MP, Collado M, Fernández PL,
Clavijo C, Navarro L, Arbona C, Marco P, Ramos-Rincon JM. (2022). Transfusion-transmitted
arboviruses: Update and systematic review. PLoS Negl Trop Dis. 16(10):e0010843. doi:
10.1371/journal.pntd.0010843.
• Goff NK, Dou T, Higgins S, Horn EJ, Morey R, McClellan K, Kurouski D, Rogovskyy AS. (2022).
Testing Raman spectroscopy as a diagnostic approach for Lyme disease patients. Front Cell Infect
Microbiol. 12:1006134. doi: 10.3389/fcimb.2022.1006134.
• Häring J, Hassenstein MJ, Becker M, Ortmann J, Junker D, Karch A, Berger K, Tchitchagua T,
Leschnik O, Harries M, Gornyk D, Hernández P, Lange B, Castell S, Krause G, Dulovic A,
Strengert M, Schneiderhan-Marra N. (2022). Borrelia multiplex: a bead-based multiplex assay for
the simultaneous detection of Borrelia specific IgG/IgM class antibodies. BMC Infect Dis.
22(1):859. doi: 10.1186/s12879-022-07863-9.
• Hoeve-Bakker BJA, Jonker M, Brandenburg AH, den Reijer PM, Stelma FF, van Dam AP, van
Gorkom T, Kerkhof K, Thijsen SFT, Kremer K. (2022). The performance of nine commercial
serological screening assays for the diagnosis of Lyme borreliosis: a multicenter modified two-gate
design study. Microbiol Spectr. 10(2):e0051022. doi: 10.1128/spectrum.00510-22.
• Hunt KM, Michelson KA, Balamuth F, Thompson AD, Levas MN, Neville DN, Kharbanda A,

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
19
Chapman L, Nigrovic LE; for Pedi Lyme Net. (2022). Racial differences in the diagnosis of Lyme
disease in children. Clin Infect Dis. ciac863. doi: 10.1093/cid/ciac863.
• Johnston D, Kelly JR, Ledizet M, Lavoie N, Smith RP, Parsonnet J, Schwab J, Stratidis J, Espich S,
Lee G, Maciejewski KR, Deng Y, Majam V, Zheng H, Bonkoungou SN, Stevens J, Kumar S,
Krause PJ. (2022). Frequency and geographic distribution of Borrelia miyamotoi, Borrelia
burgdorferi, and Babesia microti infections in New England residents. Clin Infect Dis. ciac107. doi:
10.1093/cid/ciac107.
• Karshima SN, Karshima MN, Ahmed MI. (2022). Global meta-analysis on Babesia infections in
human population: prevalence, distribution, and species diversity. Pathog Glob Health. 116(4):220-
235. doi: 10.1080/20477724.2021.1989185.
• Khan F, Allehebi Z, Shabi Y, Davis I, LeBlanc J, Lindsay R, Hatchette T. (2022). Modified two-
tiered testing enzyme immunoassay algorithm for serologic diagnosis of Lyme disease. Open
Forum Infect Dis. 9(7):ofac272. doi: 10.1093/ofid/ofac272.
• Kight E, Alfaro R, Gadila SKG, Chang S, Evans D, Embers M, Haselton F. (2022). Direct capture
and early detection of Lyme disease spirochete in skin with a microneedle patch. Biosensors
(Basel). 12(10):819. doi: 10.3390/bios12100819.
• Klingelhöfer D, Braun M, Brüggmann D, Groneberg DA. (2022). Ticks in medical and
parasitological research: Globally emerging risks require appropriate scientific awareness and
action. Travel Med Infect Dis. 50:102468. doi: 10.1016/j.tmaid.2022.102468.
• Kobayashi T, Auwaerter PG. (2022). Diagnostic testing for Lyme disease. Infect Dis Clin North
Am. 36(3):605-620. doi: 10.1016/j.idc.2022.04.001.
• Kobayashi T, Higgins Y, Melia MT, Auwaerter PG. (2022). Mistaken identity: Many diagnoses are
frequently misattributed to Lyme disease. Am J Med. 135(4):503-511.e5. doi:
10.1016/j.amjmed.2021.10.040.
• Kugeler KJ, Cervantes K, Brown CM, Horiuchi K, Schiffman E, Lind L, Barkley J, Broyhill J,
Murphy J, Crum D, Robinson S, Kwit NA, Mullins J, Sun J, Hinckley AF. (2022). Potential
quantitative effect of a laboratory-based approach to Lyme disease surveillance in high-incidence
states. Zoonoses Public Health. 69(5):451-457. doi: 10.1111/zph.12933.
• Kugeler KJ, Mead PS, Schwartz AM, Hinckley AF. (2022). Changing trends in age and sex
distributions of Lyme disease-United States, 1992-2016. Public Health Rep. (4):655-659. doi:
10.1177/00333549211026777.
• Lutaud R, Verger P, Peretti-Watel P, Eldin C. (2022). When the patient is making the (wrong?)
diagnosis: a biographical approach to patients consulting for presumed Lyme disease. Fam Pract.
cmac116. doi: 10.1093/fampra/cmac116.
• Ly DP. (2022). Black-white differences in the clinical manifestations and timing of initial Lyme
disease diagnoses. J Gen Intern Med. 37(10):2597-2600. doi: 10.1007/s11606-021-07129-1.

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
20
• Mead P. (2022). Epidemiology of Lyme disease. Infect Dis Clin North Am. 36(3):495-521. doi:
10.1016/j.idc.2022.03.004.
• Pedersen RR, Kragh KN, Fritz BG, Ørbæk M, Østrup Jensen P, Lebech AM, Bjarnsholt T. (2022).
A novel Borrelia-specific real-time PCR assay is not suitable for diagnosing Lyme
neuroborreliosis. Ticks Tick Borne Dis. 13(5):101971. doi: 10.1016/j.ttbdis.2022.101971.
• Pelletier J, Guillot C, Rocheleau JP, Bouchard C, Baron G, Bédard C, Dibernardo A, Lindsay LR,
Leighton PA, Aenishaenslin C. (2022). The added value of One Health surveillance: data from
questing ticks can provide an early signal for anaplasmosis outbreaks in animals and humans. Can J
Public Health. doi: 10.17269/s41997-022-00723-8.
• Peniche-Lara G, Moo-Salazar I, Dzul-Rosado K. (2022). A Multiplex PCR assay for a differential
diagnostic of rickettsiosis, Lyme disease and scrub typhus. J Vector Borne Dis. 59(2):178-181. doi:
10.4103/0972-9062.337506.
• Pietikäinen A, Backman I, Henningsson AJ, Hytönen J. (2022). Clinical performance and
analytical accuracy of a C6 peptide-based point-of-care lateral flow immunoassay in Lyme
borreliosis serology. Diagn Microbiol Infect Dis. 103(1):115657. doi:
10.1016/j.diagmicrobio.2022.115657.
• Pietikäinen A, Glader O, Kortela E, Kanerva M, Oksi J, Hytönen J. (2022). Borrelia burgdorferi
specific serum and cerebrospinal fluid antibodies in Lyme neuroborreliosis. Diagn Microbiol Infect
Dis. 104(3):115782. doi: 10.1016/j.diagmicrobio.2022.115782.
• Pitrak D, Nguyen CT, Cifu AS. (2022). Diagnosis of Lyme disease. JAMA. 327(7):676-677. doi:
10.1001/jama.2022.0081.
• Pratt GW, Platt M, Velez A, Rao LV. (2022). A comparison of Lyme serological testing platforms
with a panel of clinically characterized samples from various stages of Lyme disease. J Appl Lab
Med. 7(6):1445-1449. doi: 10.1093/jalm/jfac047.
• Pratt GW, Platt M, Velez A, Rao LV. (2022). Utility of whole blood real-time PCR testing for the
diagnosis of early Lyme disease. Am J Clin Pathol. 158(3):327-330. doi: 10.1093/ajcp/aqac068.
• Rodino KG, Pritt BS. (2022). When to think about other Borreliae: Hard tick relapsing fever
(Borrelia miyamotoi), Borrelia mayonii, and beyond. Infect Dis Clin North Am. 36(3):689-701. doi:
10.1016/j.idc.2022.04.002.
• Rupani A, Elshabrawy HA, Bechelli J. (2022). Dermatological manifestations of tick-borne viral
infections found in the United States. Virol J. 19(1):199. doi: 10.1186/s12985-022-01924-w.
• Sabin AP, Scholze BP, Lovrich SD, Callister SM. (2022). Clinical evaluation of a Borrelia
modified two-tiered testing (MTTT) shows increased early sensitivity for Borrelia burgdorferi but
not other endemic Borrelia species in a high incidence region for Lyme disease in Wisconsin.
Diagn Microbiol Infect Dis. 105(1):115837. doi: 10.1016/j.diagmicrobio.2022.115837.
• Sanchez-Vicente S, Jain K, Tagliafierro T, Gokden A, Kapoor V, Guo C, Horn EJ, Lipkin WI,

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
21
Tokarz R. (2022). Capture sequencing enables sensitive detection of tick-borne agents in human
blood. Front Microbiol. 13:837621. doi: 10.3389/fmicb.2022.837621.
• Schotthoefer AM, Green CB, Dempsey G, Horn EJ. (2022). The spectrum of erythema migrans in
early Lyme disease: Can we improve its recognition? Cureus. 14(10):e30673. doi:
10.7759/cureus.30673.
• Sfeir MM, Meece JK, Theel ES, Granger D, Fritsche TR, Steere AC, Branda JA. (2022).
Multicenter clinical evaluation of modified two-tiered testing algorithms for Lyme disease using
Zeus scientific commercial assays. J Clin Microbiol. 60(5):e0252821. doi: 10.1128/jcm.02528-21.
• Stellrecht KA, Wilson LI, Castro AJ, Maceira VP. (2022). Automated real-time PCR detection of
tickborne diseases using the Panther Fusion open access system. Microbiol Spectr. 10(6):e0280822.
doi: 10.1128/spectrum.02808-22.
• Tetens MM, Dessau R, Ellermann-Eriksen S, Andersen NS, Jørgensen CS, Østergaard C, Bodilsen
J, Damgaard DF, Bangsborg J, Nielsen AC, Møller JK, Omland LH, Obel N, Lebech AM. (2022).
The diagnostic value of serum Borrelia burgdorferi antibodies and seroconversion after Lyme
neuroborreliosis, a nationwide observational study. Clin Microbiol Infect. 28(11):1500.e1-1500.e6.
doi: 10.1016/j.cmi.2022.06.001.
• Theel ES. (2022). Molecular Testing for diagnosis of early Lyme disease. Am J Clin Pathol.
aqac080. doi: 10.1093/ajcp/aqac080.
• Tonnetti L, Dodd RY, Foster G, Stramer SL. (2022). Babesia blood testing: The first-year
experience. Transfusion. 62(1):135-142. doi: 10.1111/trf.16718.
• Trevisan G, Nan K, di Meo N, Bonin S. (2022). The impact of telemedicine in the diagnosis of
erythema migrans during the COVID pandemic: A Comparison with in-person diagnosis in the pre-
COVID era. Pathogens. 11(10):1122. doi: 10.3390/pathogens11101122.
• Vahey GM, Wilson N, McDonald E, Fitzpatrick K, Lehman J, Clark S, Lindell K, Pastula DM,
Perez S, Rhodes H, Gould CV, Staples JE, Cervantes K, Martin SW. (2022). Seroprevalence of
powassan virus infection in an area experiencing a cluster of disease cases: Sussex County, New
Jersey, 2019. Open Forum Infect Dis. 9(3):ofac023. doi: 10.1093/ofid/ofac023.
• Wojciechowska-Koszko I, Dziatlik J, Kwiatkowski P, Roszkowska P, Sienkiewicz M, Dołęgowska
B. (2022). Could the Optiplex Borrelia assay replace the traditional, two-step method of
diagnosing Lyme disease? Ann Agric Environ Med. 29(1):63-71. doi: 10.26444/aaem/147277.
• Wojciechowska-Koszko I, Kwiatkowski P, Sienkiewicz M, Kowalczyk M, Kowalczyk E,
Dołęgowska B. (2022). Cross-reactive results in serological tests for borreliosis in patients with
active viral infections. Pathogens. 11(2):203. doi: 10.3390/pathogens11020203.
• Wormser GP. (2022). A brief history of OspA vaccines including their impact on diagnostic testing
for Lyme disease. Diagn Microbiol Infect Dis. 102(1):115572. doi:
10.1016/j.diagmicrobio.2021.115572..

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
22
Management and Treatment
• Akoolo L, Djokic V, Rocha SC, Ulloa L, Parveen N. (2022). Sciatic-vagal nerve stimulation by
electroacupuncture alleviates inflammatory arthritis in Lyme disease-susceptible C3H mice. Front
Immunol. 13:930287. doi: 10.3389/fimmu.2022.930287.
• Allehebi ZO, Khan FM, Robbins M, Simms E, Xiang R, Shawwa A, Lindsay LR, Dibernardo A,
d'Entremont C, Crowell A, LeBlanc JJ, Haldane DJ. (2022). Lyme disease, anaplasmosis, and
babesiosis, Atlantic Canada. Emerg Infect Dis. 28(6):1292-1294. doi: 10.3201/eid2806.220443.
• Andreassen S, Lindland EMS, Beyer MK, Solheim AM, Ljøstad U, Mygland Å, Lorentzen ÅR, Reiso
H, Bjuland KJ, Pripp AH, Harbo HF, Løhaugen GCC, Eikeland R. (2022). Assessment of cognitive
function, structural brain changes and fatigue 6 months after treatment of neuroborreliosis. J Neurol.
doi: 10.1007/s00415-022-11463-7.
• Andreassen S, Solheim AM, Ljøstad U, Mygland Å, Lorentzen ÅR, Reiso H, Beyer MK, Harbo HF,
Løhaugen GCC, Eikeland R. (2022). Cognitive function in patients with neuroborreliosis: A
prospective cohort study from the acute phase to 12 months post treatment. Brain Behav. 12(6):e2608.
doi: 10.1002/brb3.2608.
• Apostolou P, Iliopoulos A, Beis G, Papasotiriou I. (2022). Supportive oligonucleotide therapy (SOT) as
a potential treatment for viral infections and Lyme disease: Preliminary results. Infect Dis Rep.
14(6):824-836. doi: 10.3390/idr14060084.
• Arnason S, Skogman BH. (2022). Effectiveness of antibiotic treatment in children with Lyme
neuroborreliosis - a retrospective study. BMC Pediatr. 22(1):332. doi: 10.1186/s12887-022-03335-w.
• Arvikar SL, Steere AC. (2022). Lyme Arthritis. Infect Dis Clin North Am. 36(3):563-577. doi:
10.1016/j.idc.2022.03.006.
• Aucott JN, Yang T, Yoon I, Powell D, Geller SA, Rebman AW. (2022). Risk of post-treatment Lyme
disease in patients with ideally-treated early Lyme disease: A prospective cohort study. Int J Infect Dis.
116:230-237. doi: 10.1016/j.ijid.2022.01.033.
• Baarsma ME, Claassen SA, van der Horst HE, Hovius JW, Sanders JM. (2022). Knowing the entire
story - a focus group study on patient experiences with chronic Lyme-associated symptoms (chronic
Lyme disease). BMC Prim Care. 23(1):139. doi: 10.1186/s12875-022-01736-5.
• Binder AM, Cherry-Brown D, Biggerstaff BJ, Jones ES, Amelio CL, Beard CB, Petersen LR, Kersh GJ,
Commins SP, Armstrong PA. (2022). Clinical and laboratory features of patients diagnosed with alpha-
gal syndrome-2010-2019. Allergy. doi: 10.1111/all.15539.
• Bloch EM, Zhu X, Krause PJ, Patel EU, Grabowski MK, Goel R, Auwaerter PG, Tobian AAR. (2022).
Comparing the epidemiology and health burden of Lyme disease and babesiosis hospitalizations in the
United States. Open Forum Infect Dis. 9(11):ofac597. doi: 10.1093/ofid/ofac597.
• Boyer PH, Lenormand C, Jaulhac B, Talagrand-Reboul E. (2022). Human co-infections
between Borrelia burgdorferi s.l. and other Ixodes-borne microorganisms: A systematic review.

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
23
Pathogens. 11(3):282. doi: 10.3390/pathogens11030282.
• Brummitt SI, Harvey DJ, Smith WA, Barker CM, Kjemtrup AM. (2022). Assessment of physician
knowledge, attitudes, and practice for Lyme disease in a low-incidence state. J Med Entomol. Sep
20:tjac137. doi: 10.1093/jme/tjac137.
• Cabello FC, Embers ME, Newman SA, Godfrey HP. (2022). Borreliella burgdorferi antimicrobial-
tolerant persistence in Lyme disease and posttreatment Lyme disease syndromes. mBio. 13(3):e0344021.
doi: 10.1128/mbio.03440-21.
• Carson AS, Gardner A, Iweala OI. (2022). Where's the beef? Understanding allergic responses to red
meat in alpha-gal syndrome. J Immunol. 208(2):267-277. doi: 10.4049/jimmunol.2100712.
• Crissinger T, Baldwin K. (2022). Early disseminated Lyme disease: Cranial neuropathy, meningitis,
and polyradiculopathy. Infect Dis Clin North Am. 36(3):541-551. doi: 10.1016/j.idc.2022.02.006.
• Dejace J. (2022). The role of the infectious disease consultation in Lyme disease. Infect Dis Clin North
Am. 36(3):703-718. doi: 10.1016/j.idc.2022.04.003.
• Delaney SL, Murray LA, Fallon BA. (2022). Neuropsychiatric symptoms and tick-borne diseases. Curr
Top Behav Neurosci. doi: 10.1007/7854_2022_406.
• Donta ST. (2022). What we know and don't know about Lyme disease. Front Public Health. 9:819541.
doi: 10.3389/fpubh.2021.819541.
• Drexler NA, Close R, Yaglom HD, Traeger M, Parker K, Venkat H, Villarroel L, Brislan J, Pastula DM,
Armstrong PA. (2022). Morbidity and functional outcomes following rocky mountain spotted fever
hospitalization-Arizona, 2002-2017. Open Forum Infect Dis. 9(10):ofac506. doi: 10.1093/ofid/ofac506.
• Dumic I, Jevtic D, Veselinovic M, Nordstrom CW, Jovanovic M, Mogulla V, Veselinovic EM, Hudson
A, Simeunovic G, Petcu E, Ramanan P. (2022). Human granulocytic anaplasmosis-a systematic review
of published cases. Microorganisms. 10(7):1433. doi: 10.3390/microorganisms10071433.
• Garro AC, Thompson AD, Neville DN, Balamuth F, Levas MN, Kharbanda AB, Bennett JE, Grant DS,
Aresco RK, Nigrovic LE; Pedi Lyme Net Network. (2022). Empiric antibiotics for children with
suspected Lyme disease. Ticks Tick Borne Dis. 13(5):101989. doi: 10.1016/j.ttbdis.2022.101989.
• Geebelen L, Lernout T, Devleesschauwer B, Kabamba-Mukadi B, Saegeman V, Belkhir L, De Munter
P, Dubois B, Westhovens R; Humtick Hospital Group, Van Oyen H, Speybroeck N, Tersago K. (2022).
Non-specific symptoms and post-treatment Lyme disease syndrome in patients with Lyme borreliosis: a
prospective cohort study in Belgium (2016-2020). BMC Infect Dis. 22(1):756. doi: 10.1186/s12879-022-
07686-8.
• Halperin JJ, Eikeland R, Branda JA, Dersch R. (2022). Lyme neuroborreliosis: known knowns, known
unknowns. Brain. 145(8):2635-2647. doi: 10.1093/brain/awac206.
• Halperin JJ. (2022). Nervous system Lyme disease-facts and fallacies. Infect Dis Clin North Am.
36(3):579-592. doi: 10.1016/j.idc.2022.02.007.

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
24
• Hill EM, Frost A. (2022). Illness perceptions, coping, and health-related quality of life among
individuals experiencing chronic Lyme disease. Chronic Illn. 18(2):426-438. doi:
10.1177/1742395320983875.
• Hoornstra D, Azagi T, van Eck JA, Wagemakers A, Koetsveld J, Spijker R, Platonov AE, Sprong H,
Hovius JW. (2022). Prevalence and clinical manifestation of Borrelia miyamotoi in Ixodes ticks and
humans in the northern hemisphere: a systematic review and meta-analysis. Lancet Microbe.
3(10):e772-e786. doi: 10.1016/S2666-5247(22)00157-4.
• Johnson LB, Maloney EL. (2022). Access to care in Lyme disease: Clinician barriers to providing care.
Healthcare (Basel). 10(10):1882. doi: 10.3390/healthcare10101882.
• Kortela E, Kanerva MJ, Kurkela S, Oksi J, Koivisto M, Järvinen A. (2022). Consumption of healthcare
services and antibiotics in patients with presumed disseminated Lyme borreliosis before and after
evaluation of an infectious disease specialist. Ticks Tick Borne Dis. 13(1):101854. doi:
10.1016/j.ttbdis.2021.101854.
• Leavey K, MacKenzie RK, Faber S, Lloyd VK, Mao C, Wills MKB, Boucoiran I, Cates EC, Omar A,
Marquez O, Darling EK. (2022). Lyme borreliosis in pregnancy and associations with parent and
offspring health outcomes: An international cross-sectional survey. Front Med (Lausanne). 9:1022766.
doi: 10.3389/fmed.2022.1022766.
• Lyons TW, Kharbanda AB, Thompson AD, Bennett JE, Balamuth F, Levas MN, Neville DN, Lewander
DP, Bretscher BS, Kellogg MD, Nigrovic LE; Pedi Lyme Net. (2022). A clinical prediction rule for
bacterial musculoskeletal infections in children with monoarthritis in Lyme endemic regions. Ann
Emerg Med. 80(3):225-234. doi: 10.1016/j.annemergmed.2022.04.009.
• MacQueen D, Centellas F. (2022). Human granulocytic anaplasmosis. Infect Dis Clin North Am.
36(3):639-654. doi: 10.1016/j.idc.2022.02.008.
• Markowicz M, Kundi M, Stanek G, Stockinger H. (2022). Nonspecific symptoms following infection
with Borrelia burgdorferi sensu lato: A retrospective cohort study. Ticks Tick Borne Dis. 13(1):101851.
doi: 10.1016/j.ttbdis.2021.101851.
• Marques A, Okpali G, Liepshutz K, Ortega-Villa AM. (2022). Characteristics and outcome of facial
nerve palsy from Lyme neuroborreliosis in the United States. Ann Clin Transl Neurol. 9(1):41-49. doi:
10.1002/acn3.51488.
• Marques A. (2022). Persistent symptoms after treatment of Lyme disease. Infect Dis Clin North Am.
36(3):621-638. doi: 10.1016/j.idc.2022.04.004.
• Marvel CL, Alm KH, Bhattacharya D, Rebman AW, Bakker A, Morgan OP, Creighton JA, Kozero EA,
Venkatesan A, Nadkarni PA, Aucott JN. (2022). A multimodal neuroimaging study of brain
abnormalities and clinical correlates in post treatment Lyme disease. PLoS One. 17(10):e0271425. doi:
10.1371/journal.pone.0271425.

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
25
• Maxwell SP, Brooks C, McNeely CL, Thomas KC. (2022). Neurological pain, psychological
symptoms, and diagnostic struggles among patients with tick-borne diseases. Healthcare (Basel).
10(7):1178. doi: 10.3390/healthcare10071178. P
• McCarthy CA, Helis JA, Daikh BE. (2022). Lyme disease in children. Infect Dis Clin North Am.
36(3):593-603. doi: 10.1016/j.idc.2022.03.002.
• Meissner HC, Steere AC. (2022). Management of pediatric Lyme disease: updates from 2020 Lyme
guidelines. Pediatrics. 149(3):e2021054980. doi: 10.1542/peds.2021-054980.
• Montero E, Gray J, Lobo CA, González LM. (2022). Babesia and human babesiosis. Pathogens.
11(4):399. doi: 10.3390/pathogens11040399.
• Murray L, Alexander C, Bennett C, Kuvaldina M, Khalsa G, Fallon B. (2022). Kundalini yoga for post-
treatment Lyme disease: A preliminary randomized study. Healthcare (Basel). (7):1314. doi:
10.3390/healthcare10071314.
• Mustafiz F, Moeller J, Kuvaldina M, Bennett C, Fallon BA. (2022). Persistent symptoms, Lyme
disease, and prior trauma. J Nerv Ment Dis. 210(5):359-364. doi: 10.1097/NMD.0000000000001452.
• Nguyen CT, Cifu AS, Pitrak D. (2022). Prevention and treatment of Lyme disease. JAMA. 327(8):772-
773. doi: 10.1001/jama.2021.25302.
• Piantadosi A, Solomon IH. (2022). Powassan virus encephalitis. Infect Dis Clin North Am. 36(3):671-
688. doi: 10.1016/j.idc.2022.03.003.
• Radesich C, Del Mestre E, Medo K, Vitrella G, Manca P, Chiatto M, Castrichini M, Sinagra G. (2022).
Lyme Carditis: From pathophysiology to clinical management. Pathogens. 11(5):582. doi:
10.3390/pathogens11050582.
• Shen RV, McCarthy CA. (2022). Cardiac manifestations of Lyme disease. Infect Dis Clin North Am.
36(3):553-561. doi: 10.1016/j.idc.2022.03.001.
• Slomski A. (2022). Shorter duration of antibiotics noninferior for Lyme disease. JAMA. 328(20):2004.
doi: 10.1001/jama.2022.21305.
• Spichler-Moffarah A, Ong E, O'Bryan J, Krause PJ. (2022). Cardiac complications of human
babesiosis. Clin Infect Dis. ciac525. doi: 10.1093/cid/ciac525.
• Strle F, Wormser GP. (2022). Early Lyme disease (erythema migrans) and its mimics (southern tick-
associated rash illness and tick-associated rash illness). Infect Dis Clin North Am. 36(3):523-539. doi:
10.1016/j.idc.2022.03.005.
• Tuvshintulga B, Sivakumar T, Nugraha AB, Ahedor B, Batmagnai E, Otgonsuren D, Liu M, Xuan X,
Igarashi I, Yokoyama N. (2022). Combination of clofazimine and atovaquone as a potent therapeutic
regimen for the radical cure of Babesia microti infection in immunocompromised hosts. J Infect Dis.
225(2):238-242. doi: 10.1093/infdis/jiab537.

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
26
• Udziela S, Biesiada G, Osiewicz M, Michalak M, Stażyk K, Garlicki A, Czepiel J. (2022).
Musculoskeletal manifestations of Lyme borreliosis - a review. Arch Med Sci. (3):726-731. doi:
10.5114/aoms.2020.96458.
• Verschoor YL, Vrijlandt A, Spijker R, van Hest RM, Ter Hofstede H, van Kempen K, Henningsson AJ,
Hovius JW. (2022). Persistent Borrelia burgdorferi sensu lato infection after antibiotic treatment:
systematic overview and appraisal of the current evidence from experimental animal models. Clin
Microbiol Rev. e0007422. doi: 10.1128/cmr.00074-22.
• Waked R, Krause PJ. (2022). Human babesiosis. Infect Dis Clin North Am. 36(3):655-670. doi:
10.1016/j.idc.2022.02.009.
• Willis SJ, Cocoros NM, Callahan M, Herrick B, Brown CM, Kruskal BA, Klompas M. (2022).
Assessment of antibiotic prescriptions for Lyme disease after modification of reporting language for
positive screening test results. JAMA Netw Open. 5(1):e2144928. doi:
10.1001/jamanetworkopen.2021.44928.
• Wong KH, Shapiro ED, Soffer GK. (2022). A review of post-treatment Lyme disease syndrome and
chronic Lyme disease for the practicing immunologist. Clin Rev Allergy Immunol. 62(1):264-271. doi:
10.1007/s12016-021-08906-w.
• Yuskevych VV, Zhulkevych IV, Makhovska OS, Smiyan SI. (2022). Assessment of quality of life in
patients with Lyme arthritis and rheumatoid arthritis. Reumatologia. 60(1):35-41. doi:
10.5114/reum.2022.114352.
Other literature relevant to tickborne diseases in Maine
• Aenishaenslin C, Charland K, Bowser N, Perez-Trejo E, Baron G, Milord F, Bouchard C. (2022).
Behavioral risk factors associated with reported tick exposure in a Lyme disease high incidence region in
Canada. BMC Public Health. 22(1):807. doi: 10.1186/s12889-022-13222-9.
• Alkishe A, Peterson AT. (2022). Climate change influences on the geographic distributional potential of
the spotted fever vectors Amblyomma maculatum and Dermacentor andersoni. PeerJ. 10:e13279. doi:
10.7717/peerj.13279.
• Al-Nazal H, Low LM, Kumar S, Good MF, Stanisic DI. (2022). A vaccine for human babesiosis:
prospects and feasibility. Trends Parasitol. 38(10):904-918. doi: 10.1016/j.pt.2022.07.005.
• Bakshi CS, Centone AJ, Wormser GP. (2022). SARS-CoV-2 is emerging in white-tailed deer and can
infect and spread among deer mice experimentally: what about deer ticks? Am J Med. 135(12):1395-1396.
doi: 10.1016/j.amjmed.2022.08.020.
• Bouchard C, Dumas A, Baron G, Bowser N, Leighton PA, Lindsay LR, Milord F, Ogden NH,
Aenishaenslin C. (2022). Integrated human behavior and tick risk maps to prioritize Lyme disease
interventions using a 'One Health' approach. Ticks Tick Borne Dis. (2):102083. doi:
10.1016/j.ttbdis.2022.102083.

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
27
• Boyce RM. (2022). Destroying the village in order to save it: Collateral damage in the battle over Lyme
disease. Open Forum Infect Dis. 9(5):ofac153. doi: 10.1093/ofid/ofac153.
• Crunkhorn S. (2022). mRNA vaccine for Lyme disease prevention. Nat Rev Drug Discov. 21(1):20. doi:
10.1038/d41573-021-00198-1.
• Dattwyler RJ, Gomes-Solecki M. (2022). The year that shaped the outcome of the OspA vaccine for
human Lyme disease. NPJ Vaccines. 7(1):10. doi: 10.1038/s41541-022-00429-5.
• Devchand R, Koehler L, Hook S, Marx GE, Hooks H, Schwartz A, Hinckley A. (2022). Understanding
consumer and clinician perceptions of a potential Lyme disease vaccine. Health Educ Res. 36(5):494-504.
doi: 10.1093/her/cyab032.
• Eisen L. (2022). Personal protection measures to prevent tick bites in the United States: Knowledge gaps,
challenges, and opportunities. Ticks Tick Borne Dis. 13(4):101944. doi: 10.1016/j.ttbdis.2022.101944.
• Eisen L. (2022). Tick species infesting humans in the United States. Ticks Tick Borne Dis. 13(6):102025.
doi: 10.1016/j.ttbdis.2022.102025.
• Elias SP, Witham JW, Schneider EF, Rand PW, Hunter ML, Lubelczyk C, Smith RP. (2022). Emergence
of Ixodes scapularis (Acari: Ixodidae) in a Small mammal population in a coastal oak-pine forest, Maine,
USA. J Med Entomol. 59(2):725-740. doi: 10.1093/jme/tjab209.
• Foster E, Burtis J, Sidge JL, Tsao JI, Bjork J, Liu G, Neitzel DF, Lee X, Paskewitz S, Caporale D, Eisen
RJ. (2022). Inter-annual variation in prevalence of Borrelia burgdorferi sensu stricto and Anaplasma
phagocytophilum in host-seeking Ixodes scapularis (Acari: Ixodidae) at long-term surveillance sites in the
upper midwestern United States: Implications for public health practice. Ticks Tick Borne Dis.
13(2):101886. doi: 10.1016/j.ttbdis.2021.101886.
• Hammond-Collins K, Tremblay M, Milord F, Baron G, Bouchard C, Kotchi SO, Lambert L, Leighton P,
Ogden NH, Rees EE. (2022). An ecological approach to predict areas with established populations of
Ixodes scapularis in Quebec, Canada. Ticks Tick Borne Dis. 13(6):102040. doi:
10.1016/j.ttbdis.2022.102040.
• Hart CE, Middleton FA, Thangamani S. (2022). Infection with Borrelia burgdorferi increases the
replication and dissemination of coinfecting powassan virus in Ixodes scapularis ticks. Viruses.
14(7):1584. doi: 10.3390/v14071584.
• Hassett E, Diuk-Wasser M, Harrington L, Fernandez P. (2022). Integrating tick density and park visitor
behaviors to assess the risk of tick exposure in urban parks on Staten Island, New York. BMC Public
Health. 22(1):1602. doi: 10.1186/s12889-022-13989-x.
• Hook SA, Hansen AP, Niesobecki SA, Meek JI, Bjork JKH, Kough EM, Peterson MS, Schiffman EK,
Rutz HJ, Rowe AJ, White JL, Peel JL, Biggerstaff BJ, Hinckley AF. (2022). Evaluating public
acceptability of a potential Lyme disease vaccine using a population-based, cross-sectional survey in high
incidence areas of the United States. Vaccine. 40(2):298-305. doi: 10.1016/j.vaccine.2021.11.065.

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
28
• Hook SA, Jeon S, Niesobecki SA, Hansen AP, Meek JI, Bjork JKH, Dorr FM, Rutz HJ, Feldman KA,
White JL, Backenson PB, Shankar MB, Meltzer MI, Hinckley AF. (2022). Economic burden of reported
Lyme disease in high-incidence areas, United States, 2014-2016. Emerg Infect Dis. 28(6):1170-1179. doi:
10.3201/eid2806.211335.
• Howard K, Beck A, Kaufman A, Rutz H, Hutson J, Crum D, Rowe A, Marx G, Hinckley A, White J.
(2022). Assessment of knowledge, attitudes, and practices toward ticks and tickborne disease among
healthcare professionals working in schools in New York and Maryland. J Sch Nurs. 10598405221099484.
doi: 10.1177/10598405221099484.
• Keesing F, Mowry S, Bremer W, Duerr S, Evans AS Jr, Fischhoff IR, Hinckley AF, Hook SA, Keating F,
Pendleton J, Pfister A, Teator M, Ostfeld RS. (2022). Effects of tick-control interventions on tick
abundance, human encounters with ticks, and incidence of tickborne diseases in residential neighborhoods,
New York, USA. Emerg Infect Dis. 28(5):957-966. doi: 10.3201/eid2805.211146.
• Laga AC, Granter SR, Mather TN. (2022). Proficiency at tick identification by pathologists and clinicians
is poor. Am J Dermatopathol. 44(2):111-114. doi: 10.1097/DAD.0000000000001977.
• Laga AC, Mather TN, Duhaime RJ, Granter SR. (2022). Identification of hard ticks in the United States:
A practical guide for clinicians and pathologists. Am J Dermatopathol. 44(3):163-169. doi:
10.1097/DAD.0000000000002005.
• Magnavita N, Capitanelli I, Ilesanmi O, Chirico F. (2022). Occupational Lyme disease: A systematic
review and meta-analysis. Diagnostics (Basel). 12(2):296. doi: 10.3390/diagnostics12020296.
• Maxwell SP, McNeely CL, Brooks C, Thomas K. (2022). Triangulating the new frontier of health geo-
data: Assessing tick-borne disease risk as an occupational hazard among vulnerable populations. Int J
Environ Res Public Health. 19(15):9449. doi: 10.3390/ijerph19159449.
• McBride SE, Lieberthal BA, Buttke DE, Cronk BD, De Urioste-Stone SM, Goodman LB, Guarnieri LD,
Rounsville TF, Gardner AM. (2022). Patterns and ecological mechanisms of tick-borne disease exposure
risk in Acadia National Park, Mount Desert Island, Maine, United States. J Med Entomol. tjac152. doi:
10.1093/jme/tjac152.
• Price KJ, Ayres BN, Maes SE, Witmier BJ, Chapman HA, Coder BL, Boyer CN, Eisen RJ, Nicholson
WL. (2022). First detection of human pathogenic variant of Anaplasma phagocytophilum in field-
collected Haemaphysalis longicornis, Pennsylvania, USA. Zoonoses Public Health. 69(2):143-148. doi:
10.1111/zph.12901.
• Raney WR, Herslebs EJ, Langohr IM, Stone MC, Hermance ME. (2022). Horizontal and vertical
transmission of powassan virus by the invasive asian longhorned tick, Haemaphysalis longicornis, under
laboratory conditions. Front Cell Infect Microbiol. 12:923914. doi: 10.3389/fcimb.2022.923914.
• Roome A, Gouli S, Yodsuwan R, Victory J, Collins C, Jenkins P, Scribani M, Krupa N, Freilich D,
Gadomski A. (2022). Tick magnets: The occupational risk of tick-borne disease exposure in forestry
workers in New York. Health Sci Rep. 5(2):e509. doi: 10.1002/hsr2.509.

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
29
• Roome A, Wander K, Garruto RM. (2022). Cat ownership and rural residence are associated with Lyme
disease prevalence in the northeastern United States. Int J Environ Res Public Health. 19(9):5618. doi:
10.3390/ijerph19095618.
• Schwartz AM, Mackeprang JM, Mead PS, Hinckley AF. (2022). Effectiveness of personal protection
measures against Lyme disease: A review of epidemiologic studies from the United States. Zoonoses
Public Health. 69(7):777-791. doi: 10.1111/zph.12984.
• Slatculescu AM, Pugliese M, Sander B, Zinszer K, Nelder MP, Russell CB, Kulkarni MA. (2022).
Rurality, socioeconomic status, and residence in environmental risk areas associated with increased Lyme
disease incidence in Ontario, Canada: A Case-Control Study. Vector Borne Zoonotic Dis. doi:
10.1089/vbz.2022.0044.
• Szewczyk-Dąbrowska A, Budziar W, Harhala M, Baniecki K, Pikies A, Jędruchniewicz N, Kaźmierczak
Z, Gembara K, Klimek T, Witkiewicz W, Nahorecki A, Barczyk K, Kłak M, Grata-Borkowska U,
Dąbrowska K. (2022). Correlation between COVID-19 severity and previous exposure of patients to
Borrelia spp. Sci Rep. 12(1):15944. doi: 10.1038/s41598-022-20202-x.
• Volk MR, Lubelczyk CB, Johnston JC, Levesque DL, Gardner AM. (2022). Microclimate conditions alter
Ixodes scapularis (Acari: Ixodidae) overwinter survival across climate gradients in Maine, United States.
Ticks Tick Borne Dis.13(1):101872. doi: 10.1016/j.ttbdis.2021.101872.
• Voyiatzaki C, Papailia SI, Venetikou MS, Pouris J, Tsoumani ME, Papageorgiou EG. (2022). Climate
changes exacerbate the spread of Ixodes ricinus and the occurrence of Lyme borreliosis and tick-borne
encephalitis in Europe-how climate models are used as a risk assessment approach for tick-borne diseases.
Int J Environ Res Public Health. 19(11):6516. doi: 10.3390/ijerph19116516.
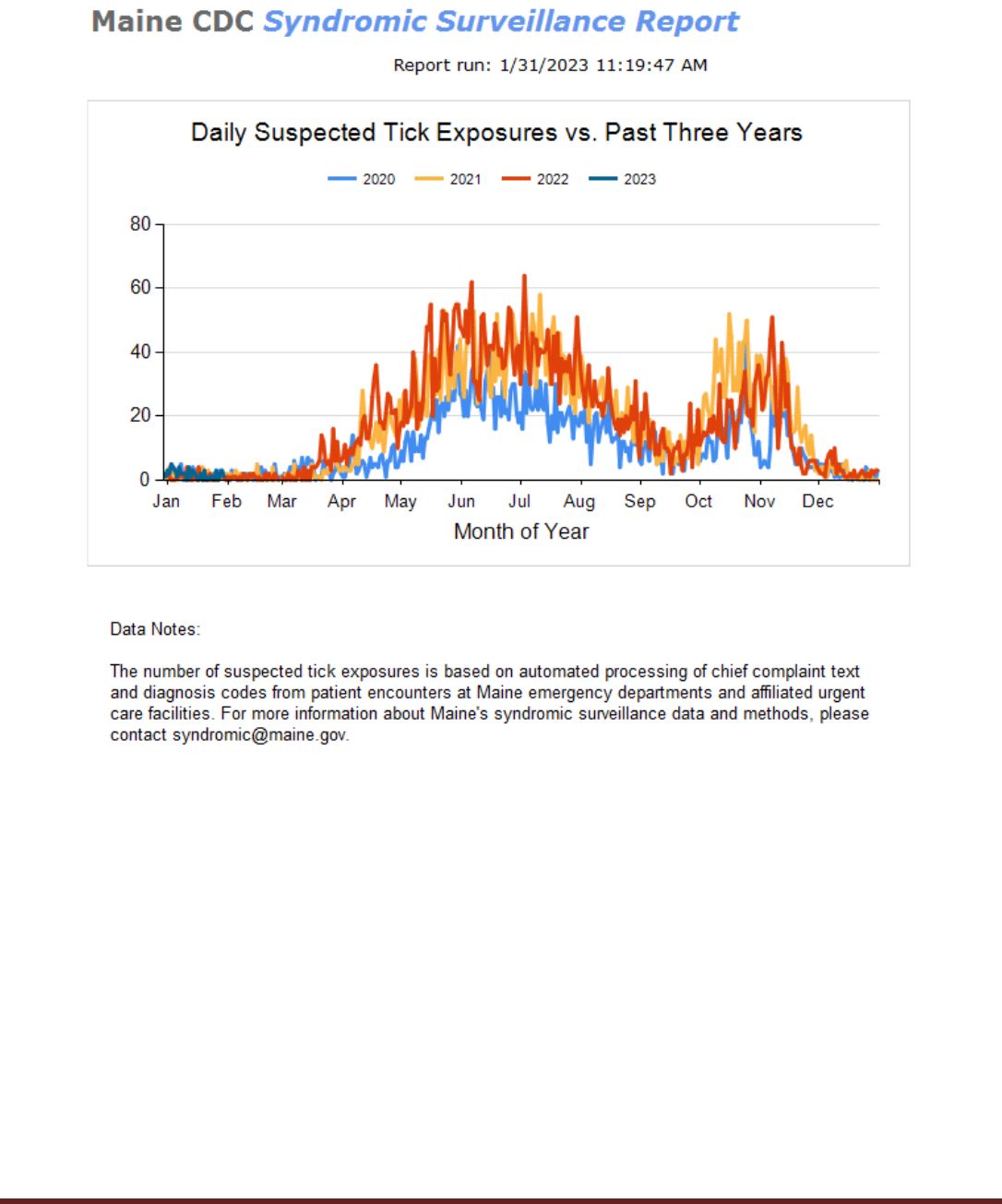
Maine CDC Report to Maine Legislature on Lyme Disease - 2023
30
Appendix 4

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
31
Appendix 5
Lyme Disease Cases per 100,000 people (Rate) – Maine, Selected years 2010-2022*
*2022 data are preliminary as of 03/08/2023

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
32
Appendix 6
Maine Vectorborne Work Group
Chair: Sara Robinson, Maine Center for Disease Control and Prevention (Maine CDC)
Bonthius, Jessica Maine CDC
Boyd, Karla Maine Board of Pesticide Control
Bryer, Pam Maine Board of Pesticide Control
Camuso, Judy Maine Department of Inland Fisheries and Wildlife
Cosenza, Danielle MaineHealth Institute for Research
Dill, Griffin Maine Cooperative Extensio
Elias, Susan MaineHealth Institute for Research, University of Maine Orono
Fish, Gary Maine Department of Agriculture, Conservation, and Forestry
Fiske, Rachael Maine Department of Agriculture, Conservation, and Forestry
Gardner, Allison University of Maine, School of Biology and Ecology
Henderson, Elizabeth MaineHealth Institute for Research
Hurwitz, Carolyn Maine Department of Agriculture, Conservation, and Forestry
Jensen, Gary Swamp, Inc.
Jensen, Rose Swamp, Inc.
Kanoti, Allison Maine Forest Service
Kantar, Lee Maine Department of Inland Fisheries and Wildlife
Lichtenwalner, Anne University of Maine, Animal Health Laboratory
Lubelczyk, Charles MaineHealth Institute for Research
Matluk, Nick Maine CDC
Meagher, Molly MaineHealth Institute for Research
Meak, Sim Maine CDC
Morris, Jesse US Department of Agriculture
Morrison, Michael Swamp, Inc.
Patterson, Megan Maine Board of Pesticides Control
Peterson, Hillary Maine Department of Agriculture, Conservation, and Forestry
Poland, Emily Maine Department of Education
Porter, Megan Maine CDC
Robich, Rebecca MaineHealth Institute for Research
Schmeelk, Thomas Maine Forest Service
Smith, Rob MaineHealth Institute for Research
Sohail, Haris Maine CDC
Staples, Joe University of Maine, Department of Environmental Science and Policy
Szantyr, Beatrice Physician, Lincoln Maine
Taylor, Tegwin Maine Department of Inland Fisheries and Wildlife
Urcuqui, Andres University of Maine, School of Forest Resources
Walsh, Michele Maine Department of Agriculture, Conservation, and Forestry
Webb, Nathan Maine Department of Inland Fisheries and Wildlife
Webber, Lori Maine CDC
To reach a member of the VBWG or to express interest in joining this workgroup, contact [email protected].

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
33
Appendix 7
2022 Governor’s Proclamation
Maine CDC Report to Maine Legislature on Lyme Disease - 2023
34
Appendix 8
Maine CDC Lyme Disease Awareness Month Poster 2022
Artwork submitted by Maisy Emery from Spruce Mountain Elementary School

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
35
Appendix 9 Maine
Tracking Network

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
36
Appendix 10
Maine Tracking Network

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
37
Appendix 11

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
38
Appendix 12
University of Maine Tick Submission and Tick Testing Data for 2022
Tick Species Submitted to the UMaine Extension Tick Lab in 2022
Source: University of Maine Cooperative Extension Tick Laboratory 2022 Annual Report
Infection Prevalence in Submitted Blacklegged (Deer) Ticks (Ixodes scapularis) in 2022
Source: University of Maine Cooperative Extension Tick Laboratory 2022 Annual Report

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
39
Infection Prevalence in Submitted American Dog Ticks (Dermacentor variabilis) and Lone Star Ticks (Amblyomma
americanum) in 2022
Source: University of Maine Cooperative Extension Tick Laboratory 2022 Annual Report
Source: University of Maine Cooperative Extension Tick Laboratory 2022 Annual Report

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
40
Appendix 13
2022 Tickborne Disease Legislation
Tickborne legislation and status recorded from LegiScan
Alabama
Title: Tickborne Illness, Commission on, extended, Act 2016-356, 2016 Reg. Sess., am'd. (HB94)
Status: Passed
Delaware
Title: Designating the Month of May 2022 as "Lyme Disease Awareness Month" in the State of Delaware (SCR99)
Status: Failed
Illinois
Title: DNR – Tick Warning Signs (HB5791)
Status: Failed
Title: Lyme Disease Awareness Month (HR0780)
Status: Passed
Massachusetts
Title: Relative to the Control of Tickborne Illness (H899)
Status: Failed
Title: Establishing a Special Commission to Find the Best Practices to Promote Education, Awareness, and Prevention
of Lyme Disease (S1500)
Status: Failed
Maryland
Title: Health Insurance – Lyme Disease and Related TickBorne Illnesses – Long–Term Antibiotic Treatment (HB1244)
Status: Failed
Maine
Title: An Act to Repeal the Pesticide Container Fee and the Tick Laboratory and Pest Management Fund (LD808)
Status: Failed
New Jersey
Title: Requires School Districts to Provide Instruction on Prevention of Lyme Disease and Other Tickborne Diseases
and to Develop Policy Concerning Removal of Ticks (A4820, S2463)
Status: Failed
Title: Requires Health Insurers to Provide Coverage for Treatment of Tickborne Diseases (S1260)
Status: Failed

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
41
New York
Title: Provides for Taxpayer Gifts for Lyme and Tickborne Diseases Education, Research and Prevention; Establishes
the Lyme and Tickborne Diseases Education, Research and Prevention Fund (S06871)
Status: Passed
Title: Provides for Taxpayer Gifts for Lyme and Tickborne Diseases Education, Research and Prevention; Establishes
the Lyme and Tickborne Diseases Education, Research and Prevention Fund (A07400)
Status: Failed
Title: Commending Delaney Dixon for Her Innovative Approach to Addressing the Lyme and Tickborne Disease Crisis
(J02633)
Status: Passed
Title: Memorializing Governor Kathy Hochul to proclaim May 2022, as Lyme Disease Awareness Month in the State of
New York (J02468, K00719)
Status: Passed
Title: Directs the Commissioner of Health to Establish a Standard Protocol for the Diagnosis and Treatment of Lyme
Disease and Other Tickborne Diseases Identified by Such Commissioner; Such Protocol Shall Require the Provision of
Written Notification to Each Patient Being Treated for Lyme Disease or Other Tickborne Diseases Relating to
Symptoms, Risk Factors, Diagnosis and Other Information Relating to Such Diseases; Enacts the "Demos Ford Act"
(S05297)
Status: Failed
Title: Includes Lyme Disease and Other Tickborne Diseases as Occupational Diseases for Purposes of Workers'
Compensation; Clarifies that Disability Includes Disability Caused by Lyme Disease or Other Tickborne Diseases
(A08614, S08867)
Status: Failed
Title: Relates to the Reporting of Lyme and Tickborne Disease Infection after Death (A04621, S00677)
Status: Failed
Title: Requires Health Insurers to Provide Coverage for Long-Term Medical Care for Lyme Disease and Other
Tickborne Related Pathogens; Provides for Taxpayer Gifts for Tickborne Illness Research, Detection and Education;
Establishes the Tickborne Illness Research, Detection and Education Fund (A01183, S00998)
Status: Failed
Title: Relates to Lyme Disease and Tickborne Infection Awareness and Prevention for Children's Overnight, Summer
Day and Traveling Summer Day Camps; Provides Guidelines for Treatment and Notification; Provides for the
Development of Materials (A07271, S03937)
Status: Failed
Title: Authorizes the Commissioner of Health to Award Grants for Graduate Medical Education in Lyme and Tickborne
Disease and to Designate Organizations as Centers for Lyme and Tickborne Disease Excellence (S02825)
Status: Failed
Title: Establishes a Pilot Program for Lyme and Tickborne Disease Testing in Children (S02148)
Status: Failed

Maine CDC Report to Maine Legislature on Lyme Disease - 2023
42
Title: Directs Promulgation of Rules and Regulations Concerning Removal of Ticks from Pupils and Notification to
Parents (S02826)
Status: Failed
Title: Directs the Superintendent of Financial Services, in Consultation with the Commissioner of Health, to Study the
Relationship between Patient Access to Care and Treatment of Lyme Disease and Health Insurance Coverage (S02822)
Status: Failed
Title: Requires Health Insurers to Provide Coverage for Long-Term Medical Care for Lyme Disease and Other
Tickborne Related Pathogen (A07495, S03896)
Status: Failed
Title: Establishes that the Council on Human Blood and Transfusion Services Shall Review all Current Medical
Research and Guidance Regarding the Donation of Blood by Patients with a History of Lyme or Tickborne Illnesses
(S02217)
Status: Failed
Title: Relates to Guidelines for Best Practices in Treating Residential Properties for Integrated Pest Management to
Assist in the Prevention of Ticks (S02946)
Status: Failed
Title: Requires the New York State Health Care Quality and Cost Containment Commission to Issue a Report
Considering the Impact on Health Insurance Costs and Quality of Legislation Requiring Coverage of Long-Term and
Chronic Lyme Disease and Other Tickborne Diseases (S03753)
Status: Failed
Pennsylvania
Title: Providing for Patient Access to Diagnostics and Treatments for Lyme Disease and Related Tickborne Illnesses;
and Requiring Health Care Policies to Provide Certain Coverage (SB1188)
Status: Failed
Title: Designating the Month of May 2022 as "Lyme Disease and Tickborne Illness Awareness Month" in Pennsylvania
(SR301)
Status: Failed
Virginia
Title: Lyme Disease; Signage in State Parks, Instructional Resources and Materials, Report (HB850)
Status: Passed
