
DOCTOR OF
NURSING PRACTICE
EDUCATION
in 2022
THE STATE OF
1
Table of Contents
INTRODUCTION .................................................................................................. 2
CONTEXT............................................................................................................. 2
I. SCOPING REVIEW OF RECENT LITERATURE ON DNP CURRICULA AND
EMPLOYMENT ................................................................................................. 4
KEY FINDINGS .................................................................................................... 4
II. REVIEW OF DNP PROGRAM CURRICULA .................................................... 4
KEY FINDINGS .................................................................................................... 5
III. KEY INFORMANT INTERVIEWS: PERSPECTIVES FROM DNP GRADUATES,
EMPLOYERS, AND ACADEMIC LEADERS ............................................................ 6
KEY FINDINGS .................................................................................................... 6
IV. DNP PROGRAM AND GRADUATE TRENDS FROM AACN SURVEY DATA ....... 9
KEY FINDINGS .................................................................................................... 9
V. SURVEY OF DNP GRADUATES’ CHARACTERISTICS, EMPLOYMENT, AND
EXPERIENCES ................................................................................................. 14
KEY FINDINGS .................................................................................................. 17
SUMMARY ........................................................................................................ 27
CONCLUSIONS................................................................................................... 28
RECOMMENDATIONS ....................................................................................... 31
REFERENCES ...................................................................................................... 32
2
Introduction
In July 2020, the Board of Directors for the American Association of Colleges of Nursing (AACN)
voted to move ahead with a new national study to assess the current state of graduates from
Doctor of Nursing Practice (DNP) programs. With a focus on nurses in practice and academia,
the study will consider the current utilization of DNP-prepared nurses, including employer,
faculty, and student perceptions of DNP preparation, as well as the impact of DNPs on patient
and system outcomes, quality of care, leadership, education, and policy development.
In September 2020, AACN issued a request for proposals and selected IMPAQ to complete the
study, which was conducted from February 2021 to February 2022. This document provides a
summary of survey findings as well as recommendations for future steps related to the practice
doctorate in nursing.
Context
In 2004, AACN released a position statement in support of the Doctor of Nursing Practice (DNP)
as the graduate degree for advanced nursing practice preparation, including but not limited to
the four advanced practice registered nurse (APRN) roles: certified registered nurse anesthetist
(CRNA), nurse practitioner (NP), clinical nurse specialist (CNS), and certified nurse-midwife
(CNM; AACN, 2004). Additionally, the Council on Accreditation of Nurse Anesthesia Educational
Programs (COA) requires that all accredited CRNA programs offer a doctoral degree for entry
into practice and, as of January 1, 2022, all students matriculating into an accredited program
must be enrolled in a doctoral program (COA, 2015). Also, in 2019, the National Organization of
Nurse Practitioner Faculties (NONPF), the leading organization for NP education, called for
moving to the DNP degree as the entry-level NP education by 2025 following a DNP summit
attended by 38 leaders from nearly 20 practice, licensure, accreditation, certification, and
educational organizations (NONPF, 2019). However, CNS and CNM organizations have not yet
called for a similar transition.
Until recently, The Essentials of Doctoral Education for Advanced Nursing Practice (AACN, 2006)
have guided the core curricula of DNP programs and competencies that DNP graduates should
have. DNP programs were initially developed using this framework. The competencies in the
original Essentials were focused on quality improvement, systems-level change, and applying
evidence-based practice. These competencies have been broadly attained as multiple surveys
have found that the majority of DNP graduates, including those with a Master of Science in
Nursing (MSN) prior to entering their DNP program, have reported that the DNP improved their
competencies in quality improvement, evidence-based practice, and leadership (Kesten et al.,
3
2022; Minnick et al., 2019). In 2021, AACN released the new Essentials, titled The Essentials:
Core Competencies for Professional Nursing Education (AACN, 2021a). The new Essentials
provide a framework for preparing individuals as members of the discipline of nursing,
reflecting expectations across the spectrum of nursing education and applied experience. These
Essentials are beginning to be implemented in schools.
Given the strong demand for the unique competencies gained by DNP graduates, the demand
for DNP education remains high and continues to grow. The number of DNP programs
increased from 156 in 2010 to 384 in 2020, and the number of enrolled DNP students increased
from 6,599 in 2010 to 35,755 in 2020. Since the completion of this study, new data from AACN
show continued growth, with the number of DNP programs increasing to 394 and the number
of enrollees in 2021 at 40,834 students (AACN, 2022). Despite this consistent increase in the
number of DNP programs and students each year since the introduction of the DNP,
approximately 90% of NPs graduated from master’s-level programs between 2019 and 2020
(AACN, 2021b).
In 2015 AACN sponsored a qualitative study conducted by the RAND Corporation, which
analyzed APRN-focused DNP programs and identified the facilitators and challenges for schools
to transition to the post-baccalaureate DNP program. Challenges included market demand,
institutional barriers, state policy and regulatory structures, university system constraints, and
resource and financial factors (Auerbach et al., 2015). In the 7 years since the publication of
that study, these challenges persist, and DNP curricula and the skill sets of DNP graduates
continue to vary. As a result, questions remain in the nursing profession, as well among
employers and the public, about variation in DNP programs, how DNP graduates are using their
education, and how the skill sets of DNP graduates differ from other graduate-prepared nurses
(McCauley et al., 2020).
This study, titled the State of Doctor of Nursing Practice Education in 2022, builds upon the
RAND study not only by updating the status of the DNP degree and providing new
recommendations 7 years later, but by performing new analyses that provide a comprehensive
picture of the DNP degree. To accomplish this goal, a mixed-methods approach was performed
with a thorough investigation of the status of the DNP degree in 2021–2022, including a
literature review; an analysis of the curricula of 50 nationally representative DNP programs; 42
key informant interviews with DNP graduates, employers, and academic leaders to gather
perceptions about DNP curricula and the skill sets and experience of DNP graduates; an analysis
of AACN survey data to provide a comprehensive picture of DNP student and program trends
between 2005 and 2020; and a survey of over 800 DNP graduates to assess a wide range of
4
topics, such as salary, satisfaction with the DNP degree, and impact of the DNP degree on their
skills and preparation for various types of employment.
The following sections provide brief summaries of and findings from each study activity and end
with conclusions and recommendations.
I. Scoping Review of Recent Literature on DNP Curricula and Employment
A scoping review was conducted of peer-reviewed and other literature published since 2015 to
assess to what extent recent relevant literature has explored DNP curricula and the
employment of DNP graduates. The research questions of the review were as follows:
1. What are the key elements of a DNP education?
2. What types of organizations do DNP graduates work for?
2a. What are their positions at those organizations?
2b. What are their roles and responsibilities in those positions?
Key Findings
● A substantial amount of literature was published between 2015 and 2021 that addressed
the research questions (17 articles for the first research question and 37 articles for the
second research question).
● The variation in DNP graduate skill sets is due primarily to the level of experience a DNP
graduate has prior to entering the DNP program.
● There is agreement among studies that the overall goal of the DNP project is to improve
quality and patient outcomes as well as achieve practice changes. However, there is
significant variability in how the DNP project is implemented among programs.
● Many articles agree that DNP graduates have great potential to impact patient and system-
level outcomes by translating evidence into practice and health policy and by using
leadership skills and interdisciplinary collaboration.
● Many DNP graduates work as direct care providers who require only a master’s degree and
therefore may not be utilizing the full scope of their DNP preparation, and they may not be
recognized for that level of education.
II. Review of DNP Program Curricula
A curriculum review was conducted to assess curriculum variability in DNP programs. The
objectives of this review were to (a) identify the range of variability in DNP programs
throughout the country, (b) assess how this variability affects DNP program quality, and (c)
5
understand how DNP program variability affects employer perceptions of the DNP skill set
versus the skill set of MSN-prepared nurses in the same area of nursing practice. The
researchers sampled 50 Commission on Collegiate Nursing Education (CCNE)-accredited
programs from the 384 nursing schools with DNP programs in 2020 and used the following
factors to assess DNP program variability: educational pathways, DNP program concentrations,
clinical placement methods, clinical site partnerships, credit hours, and DNP Project
requirements.
Key Findings
● The majority of schools in the curriculum review sample had both Bachelor of Science in
Nursing (BSN)-to-DNP and MSN-to-DNP tracks (66%), 24% had only an MSN-to-DNP track,
and 10% had only a BSN-to-DNP track.
● The majority of BSN-to-DNP programs (63%) focus on NP education, 20% on executive and
leadership education, 13% on CRNA education, and the remainder specialize in CNS
education or have a specialization in education or “advanced practice” (a generic category).
● The majority of MSN-to-DNP programs focus on NP education (28%), executive and
leadership education (28%), or are not restricted to a particular specialty (31%). Eight
percent specialize in “advanced practice” (a generic category), and the other 3% include
CNS and CRNA programs.
● For students in a BSN-to-DNP track, there was close to an even three-way split among
securing preceptorships through collaboration between schools and students (33%), giving
students the primary responsibility (31%), and giving schools the primary responsibility
(36%). In MSN-to-DNP tracks, the burden on the students to find preceptors was somewhat
greater; 39% of DNP programs require student–school collaboration, 33% place the primary
responsibility on the students, and 28% place the primary responsibility on the school.
● In our sample, the majority of DNP programs (69%) did not maintain contractual clinical site
partnerships with universities, clinics, or hospitals for guaranteed preceptorships or
graduate placement.
● On average, BSN-to-DNP tracks required 74 credit hours (with the majority being NP
concentrations). On average, MSN-to-DNP tracks required 38 credit hours. The required
number of credits may vary based on entry requirements, number of transfer credits
accepted, etc.
● All DNP programs in the sample required a DNP Project. Most schools followed AACN
recommendations that each DNP Project focuses on a change that impacts healthcare
outcomes and is related to quality improvement. There was significant variability with
6
regards to whether the project is implemented in a clinical setting; the extent to which it is
academic or policy oriented; whether secondary data analysis is permitted; and whether
the project can be carried out by a group.
● Practicum hour requirements were mostly consistent across programs, with about 500 of a
student’s required 1,000 post-baccalaureate practice hours spent practicing clinical skills
and another 500 spent working on the DNP Project. Given the wide range of DNP projects,
there is variability in the number of hours devoted to providing direct care.
III. Key Informant Interviews: Perspectives from DNP Graduates, Employers,
and Academic Leaders
Primary data was collected using in-depth interviews with the following stakeholders: DNP
graduates (14 interviews), employers of DNP graduates (13 interviews), and academic leaders
of DNP programs (15 interviews). We sought to understand the perceptions and experiences of
DNP graduates and employers regarding the value of DNP graduates in the workforce. Key
discussion topics focused on (a) the roles of DNP graduates in the workforce and how their
roles differed from those of master's-prepared nurses, (b) employer perceptions of the DNP
skill set, (c) the potential consequences of DNP program variability on the perceived value of
DNP graduates, and (d) how DNP-prepared nurses can impact patient and system outcomes.
Key Findings
● When asked about the key differences between MSN- and DNP-prepared nurses, most
graduates, employers, and academic leaders indicated that DNP graduates have a larger and
more diverse skill set—particularly in the areas of leadership, evidence-based practice,
critical thinking, and quality improvement—and greater knowledge of policy, economics,
and the business side of nursing.
● Of the 13 employers interviewed, most could not readily identify differences in the
provision of direct patient care by MSN and DNP-prepared nurses. Academic leaders could
not identify differences in clinical skills between MSN and DNP-prepared nurses. This may
relate to the fact that MSN-prepared nurses leave school having completed the same
competencies that prepare them for clinical practice.
● DNP graduates and employers expressed a lack of understanding among employers and
other healthcare professionals about the DNP degree, particularly around the skill sets of
DNP graduates, which roles they should fill, and if the goal is to produce NPs, nurse leaders,
or both.
● Academic leaders and DNP graduates provided similar views on the key differences
between BSN-to-DNP and MSN-to-DNP graduates. Academic leaders noted that differences

7
in advanced practice experience, critical thinking skills, and knowledge between these two
student groups may affect their student experiences and their post-graduation employment
opportunities. DNP graduates felt that students in MSN-to-DNP programs tend to be more
mature and to have many years of clinical and leadership experience. Graduates of the BSN-
to-DNP track are often new APRNs who do not go immediately into a leadership role but
tend to work in clinical practice.
Graduates
● When asked about their motives, most DNP graduates agreed that they were pursuing a
DNP degree to gain specialized knowledge and not necessarily expecting recognition from
their employer or a change in position. It is important to note that 13 out of 14 DNP
graduate interviewees graduated from MSN-to-DNP tracks, so their perspectives may differ
from those who graduated from BSN-to-DNP tracks.
● Many graduates discussed various challenges they encountered while completing the
program. These challenges fell into the following categories: balancing personal life and
coursework, limited time to devote to the DNP project, difficulty securing quality
preceptors, adapting to the demands of coursework or the program, and cost. The biggest
barrier they faced was balancing personal life and coursework.
● When asked about changes in roles and responsibilities, increased compensation, or other
types of employer recognition post-graduation, most DNP graduates indicated that there
was not much change to either responsibilities or salary. However, DNPs in academic roles
reported an increase in salary and responsibilities. Graduates thought that employer
perspectives on the value of the DNP skill set could be changed by changing the leadership
culture and placing more DNPs in executive positions, increasing clinical rigor within DNP
programs to increase credibility, increasing the number of DNP graduates teaching in DNP
programs, and implementing more effective marketing strategies of DNP programs.
● Graduates offered the following suggestions to improve workforce preparation: offer more
in-person (versus online) classes; focus on large-scale systems changes in the curricula;
increase the time spent gaining clinical experience; add business-related classes in areas
such as statistics, finance, communications, project management, and process
improvement; and develop professional skills needed for presentations, building a CV,
working with Microsoft programs, and career placement.
● Overwhelmingly, DNP graduates agreed that they are using evidence-based practices to
change systems and policies in their organization, which is having an impact on patient and
system outcomes.

8
Employers
● Most employers indicated that whether a DNP is required or even preferred depends on the
position. Academic employers agreed that they require a doctoral degree for faculty
positions, with some requiring a DNP specifically, and employers in hospitals or hospital
systems agreed that a DNP is usually only required for leadership and executive positions.
● Most employers want to hire candidates who understand evidence-based practice,
translate science to practice, implement quality improvement policies, and understand
systems change on a larger scale.
● A few employers noted that the student populations of BSN-to-DNP and MSN-to-DNP are
very different in general, with MSN-to-DNP students typically being older with substantially
more clinical experience. They noted that, as a result, different levels of educational support
are needed, and employers perceive that clinical experience prior to the DNP degree is an
important factor in the success of DNP graduates in applying the skills learned in the DNP
program to affect change.
● Employers offered the following suggestions on how to change perceptions of the value of a
DNP degree: increase program and DNP Project rigor, ensure that DNP graduates
demonstrate unique qualifications, change DNP marketing and communications strategies
by clearly explaining the difference between MSN and DNP skill sets, and increasing the
number of DNP graduates who publish articles.
● Of all the employers interviewed, none collected quality metrics to demonstrate the value
of the DNP. While they agreed that this was something they should do, the employers
indicated that they would have to make significant changes to their information technology
systems as they are not set up to track and monitor DNPs.
● When employers were asked how they have seen DNP graduates impact patient and system
outcomes, they mentioned graduates’ enhanced ability to implement higher level or “big
picture” thinking, implement evidence-based practice and quality improvement projects to
improve patient outcomes, and recognize system errors.
● Employers shared the following suggestions for changes to DNP curricula: increase
practicum hour requirements; limit the number of online programs; require publication of
the DNP Project; increase the focus on business education, including finance and statistics;
increase the emphasis on policy and legislation; and include social media training.

9
Academic Leaders
● Academic leaders believe that most students pursue a DNP degree for career advancement
in nursing leadership roles, advanced nursing practice, or academia. Another reason stated
was students are anticipating that an advanced degree will likely be required in the future.
● Academic leaders described several challenges that students may face in completing their
DNP degree, including working while attending graduate programs, the cost of the DNP
degree, and balancing competing life priorities. They reported that many students work full-
time while in school and that the COVID-19 pandemic has substantially increased their
workloads.
● Academic leaders reported that many DNP graduates return to the same organizations and
positions that they had before obtaining their degree. They explained that DNP graduates
often play a greater role in their organizations and that their employers occasionally provide
financial support to facilitate degree completion.
● Academic leaders expect that DNP graduates will positively impact patient outcomes at a
system level, given their leadership skills and expert knowledge in areas such as population
health and evidence-based practice.
● Academic leaders suggest that there is a need to address DNP program variability;
strengthen DNP curricula, specifically coursework in leadership, writing, communication,
finance, patient-centered care, quality, safety, and population health; include education
courses for DNP graduates pursuing an academic career; and communicate the value of the
DNP degree to key stakeholders.
IV. DNP Program and Graduate Trends from AACN Survey Data
An analysis of AACN survey data from 2005 to 2020 demonstrates how DNP program numbers
and DNP student enrollment have grown over time. Analyses of DNP student demographics,
DNP program tracks and concentrations, and associations between DNP program growth and
school characteristics are provided.
Key Findings
● The number of DNP programs and enrolled DNP students have increased every year
since the inaugural DNP programs in 2005. The number of DNP programs increased
from 156 in 2010 to 384 in 2020. Figure 1 shows the growth in DNP programs. In 2005,
only 13 schools had DNP programs; the number of DNP programs has increased steeply
every year since then. In just 5 years, between 2005 and 2010, the number of DNP
programs increased more than tenfold, from 13 to 156. Between 2010 and 2013, the
number of DNP programs continued to increase at a rapid pace, from 156 to 254. Since

10
2013, the number of DNP programs has increased every year, but at a slower pace. In
2020, there were 384 active DNP programs. The number of enrolled DNP students
increased from 6,599 in 2010 to 35,755 in 2020. In 2011, AACN reported that 867 DNP
applications were qualified but not offered admission, and in 2020, 3,664 DNP
applications were qualified but not offered admission (AACN 2012, 2021).
Figure 1: Number of Active DNP Programs 2005-2020
Note. These results differ slightly from the number of DNP programs in the annual AACN enrollment and
graduation reports because of differences in how DNP programs operated as a consortium.
● Figure 2 depicts the number of DNP programs in each state as of 2020. Each state has at
least one DNP program, with the larger number of programs concentrated in the East and in
California and Texas. The states with the highest number of DNP programs (21–30) are
Pennsylvania and Illinois.

11
Figure 2: Number of DNP Programs by State 2020
● DNP students are mostly female, although the percentage of female students is gradually
decreasing over time, from the low 90s pre-2012 to 86% in 2020.
● Figure 3 displays the racial/ethnic distribution alternatively by displaying the percentage of
all non-White students each year. Since 2006, the percentage of non-White students in DNP
programs has increased each year, from 13% in 2006 to 37% in 2020. This confirms that
racial/ethnic diversity has been increasing steadily in DNP programs. This trend seems likely
to continue, as racial/ethnic diversity has increased substantially in the last 15 years.
Figure 3: Percentage of Racial/Ethnic Minority DNP Students, 2005-2020
Note. Excludes international students and unknown/not reported race/ethnicity. Students were counted once for
each year they were in a DNP program.

12
● The number of programs that offer a BSN-to-DNP track has increased over time, but mostly
in conjunction with an increase in MSN-to-DNP tracks. In 2020, 65% of programs had both
tracks, and 30% had only an MSN-to-DNP track.
● Figure 4 presents the number of MSN-to-DNP and BSN-to-DNP students between 2005 and
2020. In 2010, 1,906 (27%) were in a BSN-to-DNP track, while the majority 5,149 (73%) were
in an MSN-to-DNP track. Between 2010 and 2020, while enrollment in tracks of both types
increased substantially, BSN-to-DNP enrollment increased at a faster pace. In 2020, 22,574
DNP students (57%) were in a BSN-to-DNP track, and 16,956 (43%) were in an MSN-to-DNP
track.
Figure 4: Number of DNP Students by Track, Excluding Direct Entry, 2005–2020
Note. Excludes students enrolled in direct entry programs, which were in the data for the first time in 2020.
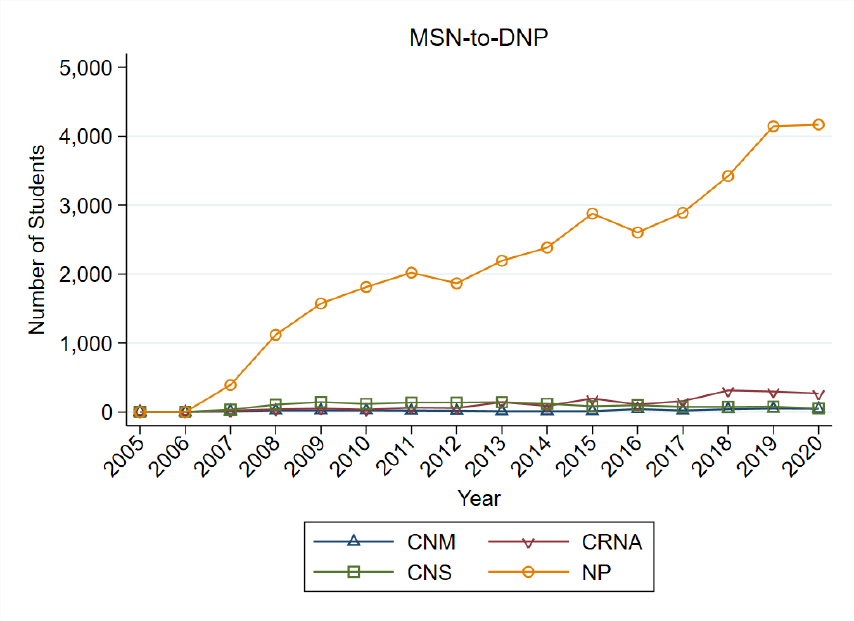
● Figures 5 and 6 show the number of DNP students in APRN programs by APRN
concentration and track. In the BSN-to-DNP track, the number of students with an NP
concentration rose rapidly in 2009, and that concentration has been the most rapidly
increasing APRN concentration ever since. However, since 2013, the number of students
with a CRNA concentration in the BSN-to-DNP track also has grown rapidly. The numbers of
BSN-to-DNP students in CNS and CNM concentrations were very small (2%) in all years. In

13
2020, there were 16,947 BSN-to-DNP students in an NP concentration (78%) and 4,341 BSN-
to-DNP students in a CRNA concentration (20%). Similarly, nearly all MSN-to-DNP students
in an APRN concentration were in an NP concentration (between 86% and 92%).
Figure 5. Number of BSN-to-DNP Students in an APRN Concentration by APRN Concentration
and Track, 2005–2020
Note. Excludes schools that wrote in one of the APRN specialties instead of selecting the appropriate APRN option
on the survey
14
Figure 6. Number of MSN-to-DNP Students in an APRN Concentration by APRN Concentration
and Track, 2005–2020
Note. Excludes schools that wrote in one of the APRN specialties instead of selecting the appropriate APRN option
on the survey. Although the majority of concentrations reported in AACN’s Enrollment and Graduation Survey data
are write-ins for the MSN-to-DNP track, only about 10% of schools had responses that contained combinations of
letters that correspond to APRNs, so the data on APRN concentrations appear to be accurate, with a relatively
small margin of error.
V. Survey of DNP Graduates’ Characteristics, Employment, and Experiences
A survey was conducted of DNP graduates online and through the mail with a sample
comprised of 875 eligible respondents, including DNP graduates working as APRNs, nurse
executives or administrators, and faculty. Questions covered DNP characteristics, employment,
and experiences, including satisfaction with the DNP degree, salary, and perceptions of specific
skills and preparation. Descriptive statistics for key data, including respondent demographics
and employment are presented. Regression analyses show how outcomes such as satisfaction
with the DNP degree, the DNP skill sets, and the perceived impact of the respondents’ DNP
education are associated with employment, school, and individual characteristics.

15
Table 1. Demographic Characteristics of DNP Survey Respondents
All respondents
Race, n (%)
White
731 (87%)
Black/African American
72 (9%)
Asian
26 (3%)
American Indian or Alaskan, Native Hawaiian or Other
Pacific Islander
a
12 (1%)
Other
34 (4%)
Hispanic or Latino origin
44 (5%)
Age category, n (%)
Age 25–34
49 (6%)
Age 35–44
134 (16%)
Age 45–54
208 (25%)
Age 55–64
310 (37%)
Age 65–100
131 (16%)
Age received DNP degree, n (%)
Age 25–34
96 (12%)
Age 35–44
177 (21%)
Age 45–54
296 (36%)
Age 55–64
239 (29%)
Age 65–100
18 (2%)
Census region of employer, n (%)
Northeast
132 (16%)
Midwest
170 (21%)
South
350 (43%)
West
153 (19%)
Advanced nursing role, n (%)
NP
274 (33%)
CRNA
69 (8%)
CNM
116 (14%)
CNS
36 (4%)
Nurse executive
211 (25%)
Other (primarily identified as a nurse educator/faculty)
127 (15%)
Primary employment position, n(%)
NP
146(18%)

16
CRNA
59 (7%)
CNM
68 (8%)
CNS
b
—
Nurse Executive
82 (10%)
Administrator
92 (11%)
Nurse faculty
187 (23%)
DNP Track, n(%)
BSN-to-DNP
110(13%)
MSN-to-DNP
498(57%)
MS-to-DNP
132 (15%)
Direct entry
73(8%)
Other
57(7%)
DNP Program Delivery, n(%)
100% online
263(30%)
100% in person
82(9%)
Blended 50% or more online
364(42%)
Blended with less than 50% online
155(18%)
Primarily Full-time versus Part-time Student, n(%)
Full-time student
488(56%)
Part-time student
372(43%)
Other
10(1%)
Note. The under 24 age category is omitted to protect privacy due to a very small sample size. The number of
respondents for each demographic characteristic varied slightly for each question because not all respondents
answered each question. Race/ethnicity percentages sum to more than 100 because survey recipients were
instructed to indicate all categories that applied.
a
Data for the categories of “American Indian or Alaskan” and “Native Hawaiian or Other Pacific Islander” were
collected separately but were combined in the reporting to protect the confidentiality of the respondents.
B
The percentages do not add to 100 for “Primary employment position” because the “Other” category is not
reported to protect the confidentiality of respondents. “—” indicates there were fewer than 10 respondents, in
which case the number was not reported to maintain confidentiality.
17
Key Findings
● Respondents were highly satisfied with their decision to obtain a DNP degree; 95% were
satisfied, including 71% who were “extremely satisfied.”
● The respondents were mostly White (87%) and over 45 years old (25% were aged 45–54,
37% were aged 55–64, and 16% were aged 65–100). A plurality (43%) was from the South.
● As with age and location, respondents had a diverse range of advanced nursing roles and
primary employment positions. The largest number of respondents were NPs (33%),
followed by nurse executives (25%), other advanced nursing roles (15%), CNMs (14%),
CRNAs (8%), and CNSs (4%). For all respondents, 33% were working in APRN roles (with the
majority working as NPs), 21% were working in an administrative or executive role, and 23%
were serving as faculty. These percentages may not be representative of the universe of
DNP graduates; they result from using professional associations to construct the sample.
● The majority of respondents graduated from a master’s-to-DNP track, with 57% in an MSN-
to-DNP track, 15% in a Master of Science (MS)-to-DNP track, and 13% in BSN-to-DNP, 8% in
direct entry program, and 7% in another track (e.g., MBA-to-DNP, MPH-to-DNP, etc.).
● As expected, the respondents who received their DNP in a master’s-to-DNP track graduated
at substantially older ages, with 40% of respondents in an MSN-to-DNP track graduating
between 45 and 54 years old and 30% graduating between 55 and 64 years old. Among
respondents in a BSN-to-DNP track, 45% graduated between 25 and 34 years old, and 33%
graduated between 35 and 44 years old. Interestingly, among respondents who received
their DNP through a direct entry program, 76% graduated between 45 and 64 years old,
similar to the percentage of respondents in master’s-to-DNP tracks who graduated in that
age range.
● Respondents working as APRNs were more involved in precepting students, and
respondents working as nurse executives precepted the fewest students. Fifteen percent of
respondents received renumeration for precepting students. The most common kind of
renumeration was a direct payment (41%), followed closely by complimentary continuing
education (39%) and less closely by an honorarium (27%). Less than 10% of respondents
received either tuition reduction or a different type of renumeration.
● Seventy-two percent of respondents attended DNP programs that were at least 50% online,
with 30% attending fully online programs and 42% attending blended programs with 50% or
more of the content online. The rest of the respondents attended fully in-person programs
(9%) or programs that were blended but less than 50% online (18%). Finally, 56% of
respondents were primarily full-time students in their DNP programs, while 43% were
primarily part-time students.

18
Regression Analysis - Regressions were used to analyze the correlations between DNP program
and individual characteristics and outcomes of interest. Outcomes of interest include
respondents’ satisfaction with their decision to obtain a DNP, skills qualified or prepared to do
after obtaining a DNP, skills improved following their DNP program, and positive impacts of
DNP education. A linear probability model was used to explore the correlations between these
outcomes and primary employment position, DNP program delivery, DNP program track,
whether the respondent was primarily a part-time or full-time student, and age. The estimates
represent associations, not causal relationships. They can be interpreted as the relationship
between characteristics and reports of skills/outcomes, conditional on other included
characteristics.
Table 2 presents a regression analysis of correlations between primary employment position,
DNP program delivery, DNP program track, whether the respondent was primarily a part-time
or full-time student, and age, with an “extremely satisfied” response to the question “How
satisfied are you with your decision to obtain a DNP degree?” The analysis was conducted using
correlations with “extremely satisfied” responses because 71% of respondents had this
response, while 94% of respondents were “extremely satisfied” or “moderately satisfied” with
their decision to obtain a DNP degree.
Respondents working as administrators (28%), nurse executives (23%), nurse faculty (14%), and
other positions (13%), relative to NPs, were more likely to be extremely satisfied with their
decision to obtain a DNP degree. Respondents primarily part-time in their DNP program were
9% less likely to be extremely satisfied with their decision to obtain a DNP degree, relative to
full-time. Respondents were increasingly extremely satisfied with their decision to obtain a DNP
degree relative to their age, with respondents aged 55 and older being significantly more likely
to be extremely satisfied than respondents under 35.
Table 2. Regression Analysis of Satisfaction With Decision to Obtain a DNP Degree
Extremely satisfied (N=764)
r(SE)
NP (Reference Category)
---
Administrator
0.28** (0.06)
CNM
-0.07 (0.07)
CRNA
-0.01 (0.07)
CNS
-0.13 (0.16)
Nurse executive
0.23** (0.06)

19
Extremely satisfied (N=764)
r(SE)
Nurse faculty
0.14** (0.05)
Other primary employment position
0.13* (0.05)
BSN-to-DNP (Reference Category)
---
MSN-to-DNP
a
0.07 (0.06)
MS-to-DNP
0.04 (0.07)
Direct entry
0.09 (0.08)
Other DNP track
-0.07 (0.08)
100% in person (Reference Category)
---
100% online DNP program
-0.05 (0.06)
Blended DNP program delivery
-0.01 (0.06)
Full-time (Reference Category)
---
Primarily part-time DNP student
-0.09** (0.03)
Other full-time or part-time status
-0.15 (0.14)
Age Under 35 (Reference Category)
---
Age 35–44
0.06 (0.08)
Age 45–54
0.09 (0.08)
Age 55–64
0.17*(0.08)
Age over 65
0.23** (0.09)
Note. A constant term is included in the regression but not reported.
* p < .05. ** p < .01.
a. While MSN-to-DNP and MS-to-DNP are modeled separately, it is recognized that these
programs are essentially the same. Note that the coefficients for the programs are similar.
20
Table 3 presents a regression analysis of correlations between primary employment position,
DNP program delivery, DNP program track, whether the respondent was primarily a part-time
or full-time student, and age, with responses to the question “Since you obtained a DNP
degree, which of the following do you feel qualified or prepared to do?” “Scholarship” is a
combination of these two sub-items: “Write for publication” and “Give presentations (regional,
national, international).” “Improved direct care” is a combination of “Provide improved direct
care services” and “Provide specialized direct care services.”
Administrators, nurse executives, nurse faculty, and other positions are more likely to be
prepared as compared to NPs to perform quality improvement and leadership activities, while
being less prepared to provide improved direct care. Nurse faculty and DNPs in other positions
are also much more likely than NPs to be prepared for scholarship activities (contributing to
publications and preparing and giving presentations). Controlling for the age of respondents,
which serves as a proxy for experience, there are no significant differences in preparation
between respondents who were in different DNP tracks, except for respondents in an MSN-to-
DNP track were significantly more likely to be prepared for scholarship activities. Respondents
who were primarily part-time DNP students felt less prepared for quality improvement and
leadership activities than respondents who were mostly full-time DNP students. Finally, for all
four categories of activities, respondents older than age 35 felt at least as well prepared as
respondents younger than age 35, with significant differences for quality improvement (age 35
and above), research (age 65 and above), and leadership (age ranges 35–44, 45–54, and 55–64).
Table 3. Regression Analysis of Activities that Respondents Feel Prepared to Do After
Obtaining a DNP Degree
Quality
improvement
(N=764)
r(SE)
Scholarship
(N=764)
r(SE)
Leadership
(N=764)
r(SE)
Improved direct
care (N=764)
r(SE)
NP (Reference Category)
---
---
---
---
Administrator
0.20**
(0.06)
0.18 (0.10)
0.21** (0.05)
-0.42** (0.12)
CNM
0.08 (0.07)
0.03 (0.11)
-0.01 (0.05)
-0.05 (0.13)
CRNA
-0.01
(0.07)
-0.08 (0.11)
-0.09 (0.06)
-0.03 (0.14)
CNS
0.26 (0.16)
0.04 (0.25)
-0.09 (0.13)
-0.07 (0.31)
Nurse executive
0.21**
(0.06)
0.11 (0.10)
0.18** (0.05)
-0.70** (0.12)
Nurse faculty
0.13*
(0.05)
0.29**
(0.08)
0.17** (0.04)
-0.51** (0.10)
21
Quality
improvement
(N=764)
r(SE)
Scholarship
(N=764)
r(SE)
Leadership
(N=764)
r(SE)
Improved direct
care (N=764)
r(SE)
Other primary employment
position
0.18**
(0.05)
0.16* (0.08)
0.14** (0.04)
-0.52** (0.10)
BSN-to-DNP (Reference
Category)
---
---
---
---
MSN-to-DNP
a
-0.02
(0.06)
0.254**
(0.09)
-0.04 (0.05)
0.03 (0.12)
MS-to-DNP
-0.05
(0.07)
0.19 (0.11)
-0.02 (0.06)
0.14 (0.14)
Direct entry
0.04 (0.08)
0.31* (0.12)
0.01 (0.06)
-0.09 (0.15)
Other DNP track
-0.08
(0.08)
0.06 (0.13)
-0.04 (0.07)
0.07 (0.17)
100% in person (Reference
Category)
---
---
---
---
100% online DNP program
0.09 (0.06)
-0.06 (0.10)
-0.01 (0.05)
-0.04 (0.12)
Blended DNP program delivery
0.07 (0.06)
0.02 (0.09)
0.01 (0.05)
0.05 (0.11)
Full-time (Reference Category)
---
---
---
---
Primarily part-time DNP
student
-0.08*
(0.03)
-0.08 (0.05)
-0.08** (0.03)
-0.04 (0.06)
Other full-time or part-time
status
-0.07
(0.14)
-0.07 (0.22)
-0.03 (0.11)
0.20 (0.28)
Age under 35 (Reference
Category)
Age 35–44
0.17*
(0.08)
0.15 (0.12)
0.20** (0.06)
0.09 (0.16)
Age 45–54
0.18*
(0.08)
0.16 (0.13)
0.19** (0.06)
0.22 (0.16)
Age 55–64
0.18*
(0.08)
0.21 (0.13)
0.18** (0.06)
0.17 (0.16)
Age over 65
0.22*
(0.09)
0.26 (0.14)
0.09 (0.07)
0.02 (0.17)
Note. A constant term is included in the regression but not reported.
* p < .05. ** p < .01.
a. While MSN-to-DNP and MS-to-DNP are modeled separately, it is recognized that these
programs are essentially the same. Note that the coefficients for the programs are similar.

22
Table 4 presents a regression analysis of correlations and (standard errors) between primary
employment position, DNP program delivery, DNP program track, whether the respondent was
primarily a part-time or full-time student, and age, with responses to the question “Which of
the following skill sets improved after obtaining your DNP degree?” The category
“Organizational change/quality improvement” is a combination of the two subitems
“Organizational change” and “Quality improvement.”
Consistent with the data on the activities respondents feel prepared to perform (as reported in
Table 3), administrators, nurse executives, and other positions were more likely than NPs to
report improvements in both policy advocacy and organizational change/quality improvement
skill sets. Respondents who had been in an MSN-to-DNP track reported larger improvements in
both skill sets than respondents who had been in a BSN-to-DNP track.
Table 4. Regression Analysis of Skill Sets That Improved After Obtaining a DNP Degree
Organizational
change/
quality improvement
(N=760)
r(SE)
Policy
advocacy
(N=760)
r(SE)
NP (Reference Category)
---
---
Administrator
0.34** (0.11)
0.18* (0.07)
CNM
-0.10 (0.12)
0.12 (0.08)
CRNA
-0.18 (0.13)
0.02 (0.08)
CNS
0.22 (0.28)
-0.14 (0.18)
Nurse executive
0.25* (0.11)
0.24** (0.07)
Nurse faculty
0.07 (0.09)
0.11 (0.06)
Other primary employment position
0.19* (0.09)
0.13* (0.06)
BSN-to-DNP (Reference Category)
---
---
MSN-to-DNP
a
0.29** (0.10)
0.15* (0.07)
MS-to-DNP
0.27* (0.12)
0.10 (0.08)
Direct entry
0.20 (0.14)
0.13 (0.09)
Other DNP track
0.06 (0.15)
0.16 (0.10)
100% in person (Reference Category)
---
---
100% online DNP program
0.14 (0.11)
0.02 (0.07)
Blended DNP program delivery
0.18 (0.10)
0.07 (0.07)
Full-time (Reference Category)
---
---
Primarily part-time DNP student
-0.01 (0.06)
-0.03 (-0.04)

23
Organizational
change/
quality improvement
(N=760)
r(SE)
Policy
advocacy
(N=760)
r(SE)
Other full-time or part-time status
0.63* (0.26)
0.20 (0.17)
Age under 35 (Reference Category)
---
---
Age 35–44 (omitted = under 35)
0.23 (0.14)
0.03 (0.09)
Age 45–54 (omitted = under 35)
0.06 (0.14)
-0.03 (0.09)
Age 55–64 (omitted = under 35)
0.06 (0.14)
0.02 (0.09)
Age over 65 (omitted = under 35)
-0.07 (0.16)
0.06 (0.10)
Note. A constant term is included in the regression but not reported.
* p < .05. ** p < .01.
a. While MSN-to-DNP and MS-to-DNP are modeled separately, it is recognized that these
programs are essentially the same. Note that the coefficients for the programs are similar.
Table 5 presents a regression analysis of correlations between primary employment position,
DNP program delivery, DNP program track, whether the respondent was primarily a part-time
or full-time student, and age, with “positive impact” responses to the question “What was the
impact, if any, on the following after obtaining a DNP degree?”
Nurse executives were, on average, 22 percentage points less likely than NPs to believe that
their preparation to work in a clinical setting improved as a result of their DNP degree.
Additionally, DNP graduates in a BSN-to-DNP track are far more likely (about 30 percentage
points on average) to have increased their preparation to practice in a clinical setting while
obtaining a DNP degree. This result may stem from two factors: 1) BSN-to-DNP graduates may
be less prepared than master’s-prepared students to practice in a clinical setting when entering
a DNP program, and 2) BSN-to-DNP tracks focus more on APRN concentrations and preparing
for clinical practice than do MSN-to-DNP tracks.
Relative to working as an NP, working as an administrator, nurse executive, or nurse faculty
member in most cases, is significantly positively associated with whether obtaining a DNP
degree impacted employment experiences (other than preparation for clinical practice). This
includes reported positive effects on how their employers assess their value, realizing
professional goals, career fulfillment, responsibilities at their place of employment, and respect
from colleagues. The only two exceptions are the impact on career fulfillment for nurse
executives and nurse faculty, as the estimates suggest there is no significant difference in the
DNP degree’s impact on their career fulfillment and its impact on the career fulfillment
experienced by NPs. The estimates for nurse executives and administrators have a larger

24
magnitude than the estimates for nurse faculty in almost all cases. CNMs are less likely than
NPs to see an impact of the DNP degree on their responsibilities and respect from colleagues,
while CRNAs are less likely than NPs to see an impact on employer assessment of their value
and career fulfillment.
Compared with being a full-time student, being primarily a part-time student is less likely to
have an impact on employer assessment of value and on career fulfillment. Finally, program
delivery (online versus in person) was not estimated to have any significant effect on any
outcomes.
Table 5. Regression Analysis of Impact on Employment Experiences After Obtaining a DNP
Degree
Preparation
to practice in
a clinical
setting
(N=755)
r(SE)
How
employer
assesses
your value
(N=759)
r(SE)
Realizing
professional
goals
(N=759)
r(SE)
Career
fulfillment
(N=760)
r(SE)
Responsibilities
at place of
employment
(N=757)
r(SE)
Respect
from
colleagues
(N=758)
r(SE)
NP
(Reference
Category)
---
---
---
---
---
---
Administra
tor
-0.05
(0.07)
0.26**
(0.07)
0.12**
(0.04)
0.12*
(0.05)
0.32**
(0.07)
0.23**
(0.06)
CNM
-0.01
(0.07)
-0.11
(0.07)
0.03
(0.05)
-0.11
(0.06)
-0.15*
(0.07)
-0.13*
(0.07)
CRNA
-0.15
(0.08)
-0.17*
(0.08)
-0.09
(0.05)
-0.14*
(0.06)
-0.02
(0.08)
-0.08
(0.07)
CNS
-0.01
(0.183)
0.21
(0.18)
-0.13
(0.12)
0.18
(0.14)
-0.04
(0.18)
0.08
(0.17)
Nurse
executive
-0.22**
(0.07)
0.25**
(0.07)
0.11*
(0.05)
0.01
(0.05)
0.26**
(0.07)
0.25**
(0.06)
Nurse
faculty
-0.02
(0.06)
0.22**
(0.06)
0.10*
(0.04)
0.06
(0.04)
0.28**
(0.06)
0.12*
(0.05)
Other
primary
employme
nt position
-0.04
(0.06)
0.12*
(0.06)
0.06
(0.04)
0.01
(0.05)
0.18**
(0.06)
0.15**
(0.05)
BSN-to-
DNP

25
Preparation
to practice in
a clinical
setting
(N=755)
r(SE)
How
employer
assesses
your value
(N=759)
r(SE)
Realizing
professional
goals
(N=759)
r(SE)
Career
fulfillment
(N=760)
r(SE)
Responsibilities
at place of
employment
(N=757)
r(SE)
Respect
from
colleagues
(N=758)
r(SE)
(Reference
Category)
MSN-to-
DNP
a
-0.35**
(0.06)
-0.04
(0.06)
-0.07
(0.04)
-0.04
(0.05)
-0.09
(0.06)
0.05
(0.06)
MS-to-DNP
-0.28**
(0.07)
-0.03
(0.07)
-0.04
(0.05)
0.00
(0.06)
-0.10
(0.07)
0.06
(0.07)
Direct
entry
-0.34**
(0.08)
-0.06
(0.08)
-0.05
(0.06)
-0.06
(0.07)
-0.17*
(0.08)
-0.01
(0.08)
Other DNP
track
-0.29**
(0.09)
-0.03
(0.09)
-0.11
(0.06)
-0.07
(0.07)
-0.20*
(0.09)
-0.04
(0.08)
100% in
person
(Reference
Category)
---
---
---
---
---
---
100%
online DNP
program
-0.12
(0.07)
-0.07
(0.07)
-0.03
(0.05)
-0.05
(0.05)
-0.13
(0.07)
0.01
(0.06)
Blended
DNP
program
delivery
-0.07
(0.06)
-0.05
(0.06)
-0.02
(0.04)
-0.06
(0.05)
-0.10
(0.06)
-0.02
(0.06)
Full-time
(Reference
Category)
---
---
---
---
---
---
Primarily
part-time
DNP
student
0.02
(0.04)
-0.08*
(0.04)
-0.03
(0.02)
-0.07*
(0.03)
0.01
(0.04)
-0.05
(0.03)
Other full-
time or
part-time
status
-0.02
(0.15)
-0.17
(0.15)
-0.23*
(0.11)
-0.13
(0.12)
-0.07
(0.15)
-0.19
(0.14)

26
Preparation
to practice in
a clinical
setting
(N=755)
r(SE)
How
employer
assesses
your value
(N=759)
r(SE)
Realizing
professional
goals
(N=759)
r(SE)
Career
fulfillment
(N=760)
r(SE)
Responsibilities
at place of
employment
(N=757)
r(SE)
Respect
from
colleagues
(N=758)
r(SE)
Age under
35
(Reference
Category)
---
---
---
---
---
---
Age 35–44
-0.04
(0.09)
-0.04
(0.09)
-0.09
(0.06)
0.06
(0.07)
0.04
(0.09)
0.04
(0.08)
Age 45–54
-0.06
(0.09)
-0.15
(0.09)
-0.02
(0.06)
0.10
(0.07)
-0.01
(0.09)
-0.05
(0.08)
Age 55–64
-0.20*
(0.09)
-0.01
(0.09)
-0.01
(0.06)
0.11
(0.07)
0.05
(0.09)
0.06
(0.08)
Age over
65
-0.16
(0.10)
-0.00
(0.09)
-0.02
(0.06)
0.16*
(0.08)
0.01
(0.10)
0.12
(0.09)
Note. A constant term is included in the regression but not reported.
* p < .05. ** p < .01.
a. While MSN-to-DNP and MS-to-DNP are modeled separately, it is recognized that these
programs are essentially the same. Note that the coefficients for the programs are similar.
27
Summary
In 2004, AACN released a position statement supporting the DNP as the graduate degree for
advanced nursing practice preparation, including but not limited to the four APRN roles. While
most of the recommendations within that report have been widely implemented, most
advanced nursing practice preparation remains at the master’s level. A qualitative study
published in 2015 by the RAND Corporation and sponsored by AACN analyzed APRN-focused
DNP programs and identified the facilitators and challenges for schools to transition to the
post-baccalaureate DNP program. Since the publication of that report, the number of DNP
programs, students, and enrollments has continued to grow rapidly.
As discussed in this report and in recent literature, DNP graduates gain unique skillsets through
their DNP education, including advanced preparation in quality improvement, evidence-based
practice, and leadership. While these skills are prevalent in DNP graduates (as they are a
universal focus of DNP programs), the experience and education of students entering DNP
programs, the curriculum of DNP programs, and perceptions of the DNP degree by DNP
graduates, employers, and academic leaders are diverse. Confusion around the DNP may stem
from the fact that the DNP education prepares graduates for a broad range of roles involving
clinical skills for direct care, quality improvement, application of evidence-based practice,
policy, research, leadership, business, and finance. This may be driven in part by the large
variation in clinical skills, experience, and professional interests of DNP students, particularly
those in BSN-to-DNP and MSN-to-DNP tracks.
The variation in program focus may lead to confusion regarding what skills DNP graduates have
and thus what value they bring to their professional positions. In particular, some employers
struggle to understand what distinguishes DNP graduates from other nurses with advanced
degrees. Conversely, many DNP graduates struggle to get their employers to understand and
recognize their unique skill sets.
This report presents the results of a variety of quantitative and qualitative activities to provide a
comprehensive picture of the state of the DNP degree and DNP graduates in 2022. Topics
include the variation in DNP curricula across a representative sample of DNP programs; how
DNP programs have grown over time and in which concentrations and tracks; who DNP
graduates are and where they are employed; and the perceptions of the DNP degree by DNP
graduates, employers of DNP graduates, and academic leaders.
28
This report shows that there is some confusion about the goals of the DNP degree and the skills
of DNP graduates across key stakeholder groups. However, there is also nearly universal
agreement that DNP graduates bring unique value in areas such as leadership, applying
evidence-based practice, quality improvement, organizational change, and process
improvement. Below, we discuss specific key findings and conclusions based on the findings in
this report.
Conclusions
The number of DNP programs and students enrolled continues to increase. The number of
DNP programs increased every year between 2005 and 2020, to a total of 384 in 2020. The
number of DNP students increased from 6,599 in 2010 to 35,755 in 2020.
Almost all DNP Survey respondents were satisfied with obtaining a DNP degree. Seventy-one
percent of DNP Survey respondents were “extremely satisfied” with their decision to obtain a
DNP degree, and 94% of respondents were either “moderately satisfied” or “extremely
satisfied.” Compared with working as an NP, working as a nurse executive, administrator, or
nurse faculty member was associated with a higher likelihood of being extremely satisfied with
the decision to obtain a DNP degree.
DNP graduates add value. As discussed in the literature and confirmed by most interviewees,
DNP graduates add unique value in areas such as evidence-based practice, organizational
change, quality improvement, and leadership. Many employer interviewees noted that DNP
graduates have an enhanced ability to “look at the big picture” and bring about change at the
organization or system level. This ability is being recognized increasingly by DNP employers
such as hospitals and hospital systems, and there is some evidence that the number of
leadership and executive positions that require or prefer a DNP is growing.
Racial/ethnic and gender diversity continues to increase. The percentage of racial/ethnic
minority students increased from 21% in 2010 to 37% in 2020. The increase in racial/ethnic
diversity is primarily due to a reduction in the number of schools having less than 20% minority
DNP students. DNP gender diversity has increased more slowly, from 9% male students in 2010
to 14% male students in 2020.
Increases in the number of DNP programs and students have occurred in both BSN-to-DNP
and MSN-to-DNP tracks. The numbers of students in BSN-to-DNP and MSN-to-DNP tracks have
increased steadily each year since 2010, and the majority of DNP students were in BSN-to-DNP
tracks in 2020. Between 2010 and 2020, the number of BSN-to-DNP students increased from
29
1,906 to 22,574, while the number of MSN-to-DNP students increased from 5,149 to 16,956.
The result Is that BSN-to-DNP students now make up the majority of DNP students, increasing
from 27% of the total in 2010 to 57% in 2020. Since 2008, nearly all of the increase in the
number of DNP programs has been in schools with both tracks.
BSN-to-DNP and MSN-to-DNP tracks have different concentrations. BSN-to-DNP tracks are
focused almost entirely on educating APRNs, while MSN-to-DNP tracks offer a wide variety of
concentrations, many focused on leadership and executive education. In our curriculum review
sample, about 30% of MSN-to-DNP tracks offered an APRN-specific concentration, while 40%
did not offer any specific concentrations, and the other 30% offered concentrations focused on
developing executive or leadership skills. In 2020, about 92% of MSN-to-DNP students in an
APRN concentration were in an NP program. In contrast, only about 78% of BSN-to-DNP
students in an APRN concentration were in an NP concentration, and nearly all the rest were in
a CRNA concentration, explained in part by the requirement that CRNAs have a DNP degree.
DNP graduates work in a variety of positions. DNP graduates are employed in a variety of
positions. Respondents to the DNP Survey were primarily employed as NPs (18%), CRNAs (7%),
CNMs (8%), CNSs (<1%), nurse executives (10%), administrators (11%), nurse faculty (23%), and
in other positions (20%). DNP graduates, employers, and academic leaders noted that the
relatively large number of DNP graduates working as faculty may be due to the fact that most
faculty positions require a nursing doctorate, and that the DNP is preferred over the PhD by
those who want to gain expertise in systems change, implementation, and leadership. Also,
some DNP graduates stated that they feel more valued in an academic setting than in a hospital
setting.
The majority of DNP programs are mostly online. Sixty-six percent of DNP programs in 2020
were mostly online, and about 72% of DNP Survey respondents attended mostly online
programs.
No evidence was found of lower quality outcomes connected to online DNP programs. We did
not find evidence that, for DNP Survey respondents, the program delivery method (online vs.
in-person) was associated with DNP skillsets, satisfaction, or their preparation to perform
various activities. Several employers perceived lower quality and rigor of online DNP programs
compared to in-person DNP programs.
DNP graduates working in administrative, executive, and faculty roles perceive higher value
from the DNP. DNP graduates who work as administrators, nurse executives, and nurse faculty
reported that they were more likely than those working as NPs to perceive their skills in
30
organizational change, quality improvement, and policy advocacy as having improved as a
result of the DNP degree. In addition, DNP graduates perceive obtaining the DNP as having had
a large impact on how their employer assesses their value, the extent to which they realize
their professional goals, their responsibilities at their place of employment, and the respect
they receive from colleagues. In most cases, these associations were larger for administrators
and nurse executives than for nurse faculty. Also, DNP Survey respondents who graduated from
an MSN-to-DNP track reported that their skills in organizational change, quality improvement,
and policy advocacy improved more than respondents who graduated from any other DNP
track.
Data do not currently exist to carry out DNP outcome studies. Data specifically on outcomes
attributed to DNP graduates versus other kinds of nurses and healthcare professionals are
required for performing DNP outcome studies. Still, our interviews with hospitals and
healthcare systems revealed that the necessary data are not currently collected. The RAND
study published in 2015 called for AACN to conduct an outcomes study to better understand
the impact of DNP graduates on patient care. We asked employers whether they collected
these data and, although they universally agreed that the data would be valuable, data sets
that would allow an outcomes study specifically on DNP graduates are not currently available.
Isolating differences in the clinical skills of MSN and DNP graduates is difficult. Almost all
graduates and employers interviewed could not identify a difference in how MSN and DNP
graduates provide direct patient care.
Uncertainty remains concerning the skills and value of DNP graduates. Despite an
understanding of the unique skills of DNP graduates by most employers, others do not
understand the value of the DNP and which roles they should fill. Some employers stated that
they were uncertain what skills DNP graduates have and what roles to put them in given
differences in the rigor, curricula, and content of DNP programs (regarding the DNP project, in
particular) and a substantial difference in the clinical experience of BSN-to-DNP and MSN-to-
DNP graduates.
Stakeholders have numerous suggestions for how to improve DNP curricula. All stakeholders
interviewed had a wide range of suggestions for how to change and improve DNP curricula.
While nearly all stakeholders agreed that DNP curricula and rigor should be standardized to
some extent, including through the assistance of accrediting bodies, they offered diverse ideas
on what should be added to DNP curricula. Suggestions included more clinical hours; post-DNP
programs similar to residencies; publication requirements for DNP projects; more leadership
and business classes (including in finance and statistics); more education on policy and
31
legislation; pedagogical training for faculty positions; and social media training. Stakeholders
held a wide variety of opinions on the skills and education they want DNP graduates to have.
Recommendations
1. Clarify the goals and identity of the DNP degree.
To increase awareness about the goals and identity of the DNP degree, clarification should be
provided regarding the purpose of the DNP degree, the roles for DNP graduates, and the skill
sets of DNP graduates.
2. Examine curriculum and rigor of DNP programs and DNP projects.
Examine DNP curricula across schools to identify hallmarks of high-quality, rigorous DNP
programs, and develop a process to encourage other schools to adopt those hallmarks.
3. Engage with APRN certification organizations.
Encourage NP, CNM, and CNS certifying bodies to require the DNP degree as the entry-to-
practice degree, as has been the model for CRNAs and other health professions that
transitioned to doctoral degree requirements.
4. Educate employers about the unique skill sets and value of DNP graduates.
Perform outreach to help employers and prospective students understand the unique
competencies and education of DNP graduates.
5. Develop processes for measuring DNP process and system-level outcome data.
Develop a plan for determining appropriate metrics and processes for collecting process and
system-level outcome data on DNP effectiveness.
6. Conduct research to isolate the impact of DNP graduates on patient and system-level
outcomes.
Once the appropriate process and outcome data have been collected, as described in the
previous recommendation, research should be conducted to isolate the impact of DNP
graduates on patient and system-level outcomes.
7. Encourage academic-practice partnerships.
Continue to enhance academic-practice partnerships to increase clinical precepting placements,
streamline the recruitment of nurses by practice partners, and help educate employers about
DNP competencies.

32
References
American Association of Colleges of Nursing. (2004). AACN position statement on the practice
doctorate in nursing. https://www.aacnnursing.org/Portals/42/News/Position-
Statements/DNP.pdf
American Association of Colleges of Nursing. (2006). The essentials of doctoral education for
advanced nursing practice [Report of the DNP Essentials Task Force].
https://www.aacnnursing.org/Portals/42/Publications/DNPEssentials.pdf
American Association of Colleges of Nursing. (2021a). The essentials: core competencies for
professional nursing education.
https://www.aacnnursing.org/Portals/42/AcademicNursing/pdf/Essentials-2021.pdf
American Association of Colleges of Nursing. (2021b). 2020–2021 enrollment and graduations
in baccalaureate and graduate programs in nursing.
https://www.aacnnursing.org/News-Information/Research-Data-Center/Standard-Data-
Reports
American Association of Colleges of Nursing. (2022). 2021-2022 enrollment and graduations in
baccalaureate and graduate programs in nursing. https://www.aacnnursing.org/News-
Information/Research-Data-Center/Standard-Data-Reports
American Association of Colleges of Nursing. (2005-2021). Institutional Data Services Custom
Reports.
Auerbach, D. I., Martsolf, G. R., Pearson, M. L., Taylor, E. A., Zaydman, M., Muchow, A. N.,
Spetz, J., & Lee, Y. (2015). The DNP by 2015: A study of the institutional, political, and
professional issues that facilitate or impede establishing a post-baccalaureate doctor of
nursing practice program. RAND Corporation.
https://www.rand.org/pubs/research_reports/RR730.html
Council on Accreditation of Nurse Anesthesia Educational Programs. (2015). Standards for
accreditation of nurse anesthesia programs practice doctorate.
https://www.coacrna.org/wp-content/uploads/2020/01/Standards-for-Accreditation-
of-Nurse-Anesthesia-Programs-Practice-Doctorate-revised-October-2019.pdf
33
Kesten, K. S., Moran, K., Beebe, S. L., Conrad, D., Burson, R., Corrigan, C., Manderscheid, A., &
Pohl, E. (2021). Drivers for seeking the doctor of nursing practice degree and
competencies acquired as reported by nurses in practice. Journal of the American
Association of Nurse Practitioners, 34(1), 70–78.
https://doi.org/10.1097/JXX.0000000000000593
McCauley, L. A., Broome, M. E., Frazier, L., Hayes, R., Kurth, A., Musil, C. M., Norman, L. D.,
Rideout, K. H., & Villarruel, A. M. (2020). Doctor of nursing practice (DNP) degree in the
United States: Reflecting, readjusting, and getting back on track. Nursing Outlook, 68(4),
494–503. https://doi.org/10.1016/j.outlook.2020.03.008
Minnick, A. F., Kleinpell, R., & Allison, T. L. (2019). DNP graduates’ labor participation, activities,
and reports of degree contributions. Nursing Outlook, 67(1), 89–100.
https://doi.org/10.1016/j.outlook.2018.10.008
National Organization of Nurse Practitioner Faculties. (2019). The Doctor of Nursing Practice
Summit: Update summary from workgroups, August 14, 2019.
https://cdn.ymaws.com/www.nonpf.org/resource/resmgr/dnp/20190814_dnp_summit
_workgrou.pdf
